Download
1 / 7
70 likes | 84 Views
This project aims to reduce post-operative venous thromboembolism rates at LUMC by 50%. Team members from Surgery, Nursing, General Medicine, and Pharmacy collaborated to develop a risk assessment tool and guideline for VTE prophylaxis. The initiative includes piloting the tools in the Department of Surgery, monitoring their use, and implementing them in Orthopaedic Surgery and Neurosurgery. The strategy involves evaluating prophylaxis methods based on risk stratification and national guidelines to improve patient outcomes.

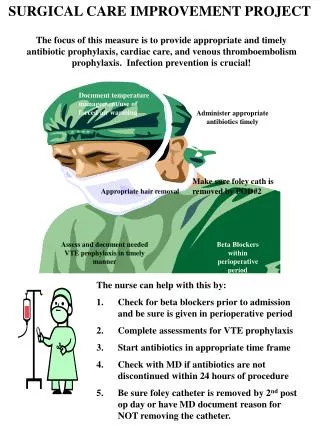
E N D
Surgical Care Improvement Project Prevention of Post-operative Venous Thromboembolism Team Membership Department of Surgery, Nursing, General Medicine, Pharmacy, CCE
Opportunity Statement • Venous thromboembolism (VTE- deep vein thrombosis and pulmonary embolism) is the most common preventable cause of death following surgery. • The rate of post-operative VTE at LUMC (2-3%) is at the 90th percentile compared to other Academic Medical Centers (UHC data)
Post-operative pulmonary embolism or deep vein thrombosis 3.0 2.5 2.0 Rate per 100 cases 1.5 1.0 0.5 2002 Q1 2002 Q2 2002 Q3 2002 Q4 2003 Q1 2003 Q2 2003 Q3 2003 Q4 2004 Q1 2004 Q2 2004 Q3 2004 Q4 2005 Q1 2005 Q2 2005 Q3 Quarter LUHS Rate UHC Ninetieth Percentile UHC Median UHC Tenth Percentile
Project Goals • Achieve a 50% reduction in the occurrence rate of post-operative venous thromboembolism
Most Likely Causes for Current Opportunity • Surgical patients are not routinely assessed and stratified for VTE risk • Wide variability in use of prophylactic methods • Variable awareness of national, evidence-based guidelines* • Under utilization of pharmacologic prophylaxis (heparin) * Geerts, WH et al. Prevention of venous thromboembolism: The Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest 2004;126:338s-400s.
Solutions Planned • Developed Risk Assessment Tool(see figure 1) • Developed guideline for selection of appropriate VTE prophylaxis for surgical patients(see figure 1) • Contacted Best Practice Academic Medical Centers
Next Steps • Pilot Risk Assessment Tool and Guideline in Department of Surgery • Monitor use of risk assessment tool • Evaluate the use of mechanical and pharmacologic based upon risk stratification and prophylaxis guidelines • Implement Risk Assessment Tool and Prophylaxis Guideline in Orthopaedic Surgery and Neurosurgery • Continue comparison with UHC data