Download

1 / 18
250 likes | 883 Views
Surgical Care Improvement Project (SCIP). CURRENT SCIP MEASURES. SCIP-1 Pre-op Antibiotic given within 1 hr. before incision SCIP-2 Must receive SCIP recommended prophylactic antibiotic SCIP-3 Discontinue antibiotic within 24 hrs. of anesthesia end time

E N D
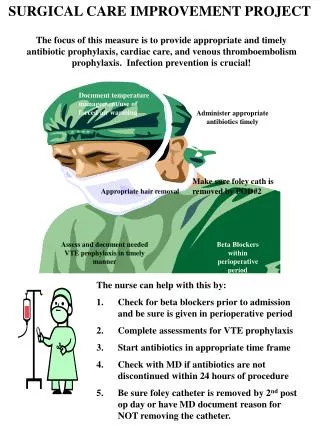
CURRENT SCIP MEASURES • SCIP-1Pre-op Antibiotic given within 1 hr. before incision • SCIP-2Must receive SCIP recommended prophylactic antibiotic • SCIP-3 Discontinue antibiotic within 24 hrs. of anesthesia end time (cardiac op exception) • SCIP-4 Controlled 6 am postoperative serum glucose (cardiac only) • SCIP-6 Appropriate hair removal • SCIP-CARD-2 Perioperative beta-blocker therapy for pre B blocker Rx • SCIP-VTE-2 VTE prophylaxis within 24 hrs. prior to or after anesthesia end time • SCIP-9 Removeurinary catheter by postop day 2 • SCIP-10 Temperature >96.8 F- 15 min. after anesthesia end time
SCIP-1-2-3 AntibioticsAppropriate, Pre-incision Timing, D/C Time Antibiotics 1. Given on time: 1 hour before incision, 2 hrs – Vancomycin& Levaquin 2. Appropriate selection of antibiotic-seeguidelines sheet 3. Discontinued within 24 hour after anesthesia end time (exception: 48 hours for cardiovascular surgery) Provider must document reason to extend if applicable, i.e.: infection, suspected infection Why: Antibiotic must be present at time of fibrin formation (at surgical incision) for effectiveness. Cephalosporins have broad spectrum of activity against both gram-positive and gram- neg bacteria and wide range of therapeutic to toxic dosage. Cephalosporin's are inexpensive and easy to administer, and allergic reactions are rare. After an incision is closed, antibiotics have no appreciable effect of preventing infections.
If Using Vanco **If Vancomycin is marked on the physician order and patient does NOT have any allergies, one of the following needs to be documented : • MRSA, Colonization or infection • Patient with an acute inpatient hospitalization within the last year • Patient residing in a nursing home within the last year • Patient with chronic wound care or dialysis • Patient with continuous inpatient stay more than 24 hours prior to the principal procedure • Patient transferred from another inpatient hospitalization after a 3 day stay • Patient undergoing valve surgery
Re-dosing **Levofloxacin, gentamicin, ertapenem, and metronidazole do NOT need to be re-dosed at any time intraoperatively *Re-dosing recommendations come from 2012 Infectious Disease Society of America (IDSA) Recommendations
SCIP-4 Blood Glucose < 200 • Blood Glucose (CV has it in their guidelines) Cardiac surgery patients – controlled 6AM postoperative serum glucose (less than 200 mg/dl postop day 1 and 2) Why? Risk of infections higher if blood glucose levels elevated
SCIP-6 Hair Removal • Hair Removal Clippers in OR only-no other option Why? Shaving with a razor causes skin abrasions which may lead to infections.
SCIP-9 Foley D/C • Urinary Catheter Discontinued by postop day 2 Or physician, PA, APN documented reason to continue beyond day 2-i.e.: pts. with urologic, gyne, perineal op, I&O Why? Risk of urinary tract infection (UTI) with > use of urinary catheter
SCIP-Cardiac-2 Beta Blocker • Beta Blocker • Continue if patient on home beta blocker therapy • Beta blocker may be given 24 hrs. prior to op or day of procedure (up to 12 midnight) heart rate must be ≥ 50 and systolic blood pressure ≥ 100 If held according to parameters, physician, PA, APN reason must be documented • Then Beta blocker continued postop days 1 & 2 (Physician, PA, APN documented reason if held postop) Why? Perioperative myocardial ischemia has been identified as the #1 risk factor for mortality after non-cardiac surgery. This is attributed to the exaggerated sympathetic response leading to persistently elevated heart rate. Has the potential to significantly reduce cardiac deaths for up to 2 years postoperatively!
SCIP-VTE-2 Timing Of VTE Prophylaxis VTE (Venous Thromboembolism) Prophylaxis • Mechanical and/or pharmacological prophylaxis is ordered according to VTE risk assessment tool and type of surgery • Prophylaxis is given 24 hrs. prior to surgery or within 24 hours after anesthesia end time • (guidelines on back of checklist) Provider documentation required if contraindicated : i.e. open wound, bleeding risk. Why? Reduces the risk of development of pulmonary embolism and DVT
SCIP-10 Normothermia • Temperature Management At least ≥ 96.8°F/36°C within 15 minutes of anesthesia end time or warmer used in OR Exception: Provider documentation of intentional hypothermia Why? 3 times greater incidence of surgical site infections with hypothermia Delayed wound closure which results in prolonged hospitalization
We Can’t Afford Even One Miss!! We CAN achieve our goal of 100% compliance if we ALL work together to make it happen!