Download
1 / 1
10 likes | 188 Views
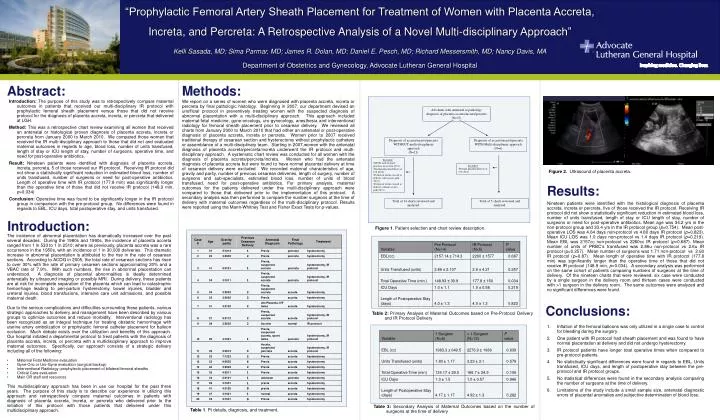
“Prophylactic Femoral Artery Sheath Placement for Treatment of Women with Placenta Accreta, Increta, and Percreta: A Retrospective Analysis of a Novel Multi-disciplinary Approach”

E N D
“Prophylactic Femoral Artery Sheath Placement for Treatment of Women with Placenta Accreta, Increta, and Percreta: A Retrospective Analysis of a Novel Multi-disciplinary Approach” Kelli Sasada, MD; Sima Parmar, MD; James R. Dolan, MD; Daniel E. Pesch, MD; Richard Messersmith, MD; Nancy Davis, MA Department of Obstetrics and Gynecology, Advocate Lutheran General Hospital Abstract: Methods: Introduction: The purpose of this study was to retrospectively compare maternal outcomes in patients that received our multi-disciplinary IR protocol with prophylactic femoral sheath placement versus those that did not receive protocol for the diagnosis of placenta accreta, increta, or percreta that delivered at LGH. Method: This was a retrospective chart review examining all women that received an antenatal or histological proven diagnosis of placenta accreta, increta or percreta from January 2000 to March 2010. We compared those women that received the IR multi-disciplinary approach to those that did not and evaluated maternal outcomes in regards to age, blood loss, number of units transfused, length of stay or ICU length of stay, number of surgeons, operative time, and need for post-operative antibiotics. Result: Nineteen patients were identified with diagnosis of placenta accreta, increta, percreta, 5 of those received our IR protocol. Receiving IR protocol did not show a statistically significant reduction in estimated blood loss, number of units transfused, number of surgeons or need for post-operative antibiotics. Length of operative time with IR protocol (177.8 min) was significantly longer than the operative time of those that did not receive IR protocol (148.9 min, p=0.034) Conclusion: Operative time was found to be significantly longer in the IR protocol group in comparison with the pre-protocol group. No differences were found in regards to EBL, ICU days, total postoperative stay, and units transfused. We report on a series of women who were diagnosed with placenta accreta, increta or percreta by final pathologic histology. Beginning in 2007, our department devised an unofficial protocol in preventively treating women with the suspected diagnosis of abnormal placentation with a multi-disciplinary approach. This approach included maternal-fetal medicine, gyne-oncology, uro-gynecology, anesthesia and interventional radiology for femoral sheath placement prior to cesarean delivery. We reviewed all charts from January 2000 to March 2010 that had either an antenatal or post-operative diagnosis of placenta accreta, increta or percreta. Women prior to 2007 received traditional therapy of cesarean section and hysterectomy without prophylactic catheters or assemblance of a multi-disciplinary team. Starting in 2007,women with the antenatal diagnosis of placenta accreta/percreta/increta underwent the IR protocol and multi-disciplinary approach. A systematic chart review was conducted for all women with the diagnosis of placenta accreta/percreta/increta. Women who had the antenatal diagnosis of placenta accreta but were found to have normal placental delivery at time of cesarean delivery were excluded. We recorded maternal characteristics of age, gravity and parity, number of previous cesarean deliveries, length of surgery, number of surgeons and sub-specialists, estimated blood loss, number of units of blood transfused, need for post-operative antibiotics. For primary analysis, maternal outcomes for the patients delivered under this multi-disciplinary approach were compared to those that delivered prior to the implementation of this protocol. A secondary analysis was then performed to compare the number surgeons at the time of delivery with maternal outcomes regardless of the multi-disciplinary protocol. Results were reported using the Mann-Whitney Test and Fisher Exact Tests for p-values. All charts with antenatal or pathology diagnosis of placenta accreta/increta/percreta (N=27) Diagnosis of accreta/increta/percreta WITHOUT multi-disciplinary approach (N=21) Diagnosis of accreta/increta/percreta WITH Multi-disciplinary approach (N=6) • Excluded: • NSVD with retained placenta, no accreta (N=1) • Normal placenta delivery at C/S (N=4) • Portion of uterus excised at delivery with accreta path (N=1) • Portion of uterus excised at delivery without accreta path (N=1) • Excluded: • Normal placenta delivery at C/S (N=1) Figure 2. Ultrasound of placenta accreta. Results: Total of 14 charts reviewed and analyzed. Total of 5 charts reviewed and analyzed. Nineteen patients were identified with the histological diagnosis of placenta accreta, increta or percreta, five of those received the IR protocol. Receiving IR protocol did not show a statistically significant reduction in estimated blood loss, number of units transfused, length of stay or ICU length of stay, number of surgeons or need for post-operative antibiotics. Mean age was 34.2 yrs in the non-protocol group and 33.4 yrs in the IR protocol group (p=0.754). Mean post-operative LOS was 4.64 days non-protocol vs 4.80 days IR protocol (p=0.823). Mean ICU LOS was 1.0 days non-protocol vs 1.4 days IR protocol (p=0.219). Mean EBL was 2157cc non-protocol vs 2260cc IR protocol (p=0.687). Mean number of units of PRBC’s transfused was 2.86u non-protocol vs 2.6u IR protocol (p=0.257). Mean number of surgeons was 1.71 non-protocol vs 2.60 IR protocol (p=0.87). Mean length of operative time with IR protocol (177.8 min) was significantly longer than the operative time of those that did not receive IR protocol (148.9 min, p=0.034). A secondary analysis was performed on the same cohort of patients comparing numbers of surgeons at the time of delivery. Of the nineteen charts that were reviewed, six case were conducted by a single surgeon in the delivery room and thirteen cases were conducted with >1 surgeon in the delivery room. The same outcomes were analyzed and no significant differences were found. Introduction: Figure 1. Patient selection and chart review description. • The incidence of abnormal placentation has dramatically increased over the past several decades. During the 1980s and 1990s, the incidence of placenta accreta ranged from 1 in 533 to 1 in 2510; where as previously, placenta accreta was a rare occurrence in the 1950s, with an incidence of 1 in 30,000 deliveries. This dramatic increase in abnormal placentation is attributed to the rise in the rate of cesarean sections. According to ACOG in 2005, the total rate of cesarean sections has risen to over 30% with the rate of primary cesarean sections approximating 20% and a VBAC rate of 7.9%. With such numbers, the rise in abnormal placentation can understood. A diagnosis of placental abnormalities is ideally determined antenatally by ultrasound imaging or possibly MRI. During delivery, these patients are at risk for incomplete separation of the placenta which can lead to catastrophic hemorrhage leading to peri-partum hysterectomy, bowel injuries, bladder and ureteral injuries, blood transfusions, intensive care unit admissions, and possible maternal death. • Due to the serious complications and difficulties surrounding these patients, various strategic approaches to delivery and management have been described by various groups to optimize outcomes and reduce morbidity. Interventional radiology has been recognized as an integral technique for treating obstetric hemorrhage with uterine artery embolization or prophylactic femoral catheter placement for balloon occlusion. Much debate exists over the utilization and benefits of this approach. Our hospital initiated a departmental protocol to treat patients with the diagnosis of placenta accreta, increta, or percreta with a multidisciplinary approach to improve maternal outcomes. Specifically, our approach consists of a strategic delivery including all of the following: • Maternal Fetal Medicine evaluation • Gyne-Onc or Uro-Gyne evaluation (surgical backup) • Interventional Radiology: prophylactic placement of bilateral femoral sheaths • Critical Care evaluation • Main OR staff and resources • This multidisciplinary approach has been in use our hospital for the past three years. The purpose of this study is to describe our experience in utilizing this approach and retrospectively compare maternal outcomes in patients with diagnosis of placenta accreta, increta, or percreta who delivered prior to the initiation of this protocol with those patients that delivered under this multidisciplinary approach. Conclusions: Table 2: Primary Analysis of Maternal Outcomes based on Pre-Protocol Delivery and IR Protocol Delivery Inflation of the femoral balloons was only utilized in a single case to control for bleeding during the surgery. One patient with IR protocol had sheath placement and was found to have normal placentation at delivery and did not undergo hysterectomy. IR protocol patients have longer total operative times when compared to pre-protocol patients. No statistically significant differences were found in regards to EBL, Units transfused, ICU days, and length of postoperative stay between the pre-protocol and IR protocol groups. No statistical differences were found in the secondary analysis comparing the number of surgeons at the time of delivery. Limitations of the study include a small sample size, antenatal diagnostic errors of placental anomalies and subjective determination of blood loss. Table 3: Secondary Analysis of Maternal Outcomes based on the number of surgeons at the time of delivery Table 1. Pt details, diagnosis, and treatment.