Download
1 / 32
340 likes | 637 Views
T he Role of ACEIs in Unstable Angina. Sukhjinder Sidhu Interior Health Pharmacy Resident Cardiology Rotation February 21, 2014. Learning Objectives. By the end of this 20-min session the audience should be able to:

E N D
The Role of ACEIs in Unstable Angina Sukhjinder Sidhu Interior Health Pharmacy Resident Cardiology Rotation February 21, 2014
Learning Objectives • By the end of this 20-min session the audience should be able to: • Describe the pathophysiology and clinical presentation of unstable angina (UA) • Compare and contrast the diagnostic criteria of UA, NSTEMI and STEMI • State the evidence for ACEI in UA • Be able to determine the need for ACEI in an UA patient
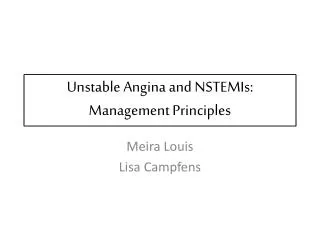
LAD RCA LCA Cx
DRP’s • BL is at risk of recurrent MI and death secondary to not receiving an ACEI and would benefit from optimization of ACS therapy. • BL is at risk of experiencing recurrent MI and death secondary to smoking and would benefit from smoking cessation. • BL is at risk of experiencing recurrent MI, worsening heart function and death secondary to ibuprofen use and would benefit from discontinuing ibuprofen and counseling on its adverse effects. • BL is at risk of experiencing influenza(fever, night sweats, myalgias, fatigue, nausea, vomiting, diarrhea) secondary to not receiving an influenza vaccine and would benefit from receiving the influenza vaccine. • BL is experiencing a mild rash secondary to the adhesives on the ECG strips and nicotine patch and would benefit from receiving a topical corticosteroid formulation.
Unstable Angina • Angina is caused by poor blood flow through the coronary vessels of the myocardium • Acute reduction in myocardial oxygen supply • CAD due to atherosclerosis is the most common cause of UA heartcurrents.com
Goals of Therapy • Prevent mortality • Minimize myocardial damage and total ischemic time • Establish and maintain patency of the infarct-related artery • Alleviate signs and symptoms • Prevent re-occlusion, re-infarction, re-hospitalization • Minimize adverse events • Promote smoking cessation
Therapeutic Approach • ASA 81 mg PO daily • P2Y12 inhibitors • High dose statin • Beta-blockers • RAAS inhibitors • Nitroglycerin PRN
RAAS Inhibitors • Improve vascular endothelial function • Inhibit hypertrophy • Increase bradykinin • Increases nitric oxide production = vasodilation • Anti-atherosclerotic effects • Antagonize the rupture of plaques • Enhance fibrinolysis • Blood pressure control
Background • ACC/AHA Guidelines for UA/NSTEMI • ACEI should be given and continued indefinitely for patients recovering from UA/NSTEMI with HF, LV dysfunction, HTN, or DM, unless contraindicated (Class I A) • ACEIs have been shown to reduce mortality rates in patients with AMI and in patients with recent MI or with LV systolic dysfunction, in diabetic patients with LV dysfunction, and in a broad spectrum of patients with high-risk chronic CAD • ACEI are reasonable for patients recovering from UA/NSTEMI in the absence of LV dysfunction, HTN, or DM, unless contraindicated (Class IIa B) ACC/AHA 2007 Guidelines for UA/NSTEMI
NEJM 2000 342:3;145-33, LANCET 2003 362;782-88, NEJM 2004; 351:205-68
NEJM 2000 342:3;145-33, LANCET 2003 362;782-88, NEJM 2004; 351:205-68
IMAGINE Circulation. 2008; 117:24-31
IMAGINE Circulation. 2008; 117:24-31
IMAGINE • Author’s conclusions: • At least in low risk-patients treated with contemporary therapy, early initiation of an ACEI after CABG has no benefit, and this strategy may even be associated with an increase in adverse events Circulation. 2008; 117:24-31
IMAGINE • Strengths • High compliance • Large number of patients receiving appropriate cardiac medications • Limitations • 11% of placebo cohort was taking open-label ACEI at 3 years • Industry sponsored • Generalizability • Patient had CABG surgery • Normal LVEF • Excluded majority of DM patients Circulation. 2008; 117:24-31
Application • Necessary • No prior risk factors, such as DM, HTN or ↓ LVEF • Effective • In CABG patients with no clear indication for ACEI, they have conflicting evidence in reducing CV death, non-fatal MI, and revascularization • Safety • Risk of hypotension and cough • BP was consistently 95-110/60-70 • Adherence • Minimal non-adherence risk • Patient Factors • Increased pill and cost burden
Therapeutic Plan • Do not initiate an ACEI at present • Administer influenza vaccine 0.5 mL IM x 1 • Hydrocortisone cream 1% apply to affected areas BID PRN • Provided counseling regarding A/E of NSAID use • Provided counseling on the use of acetaminophen over NSAIDs for OA pain • Provided counseling and reinforcement regarding smoking cessation
Follow Up • ACEI not initiated at this time • Influenza vaccine administered • BL receptive to smoking cessation • BL receptive to avoiding use of NSAIDs and using acetaminophen for pain control • Successful CABG
Conclusion • No studies have evaluated ACEI solely in UA patients • ACEI decreased CV death and non-fatal MI in CAD patients if other risk factors are present • HTN, DM, ↑ chol, or ↓ LVEF • ACEI have not shown similarly consistent results in lower CV risk patients
NSAIDs & CV Risk • COX-1 is active in platelets - Thromboxane A2 is a vasoconstrictor and potent stimulator of platelet aggregation- TXA2 increases renal salt & fluid retention, increases BP, enhances MI & vascular remodeling • COX-2 is active in cells that line blood vessels - Prostacyclin is a potent vasodilator and inhibitor of platelet function = vasculoprotective- PGI2 facilitates renal salt & fluid excretion, lowers BP- inhibition decreases prostacyclin- Endothelial cells are a source of prostacyclin • NSAIDs tip the TXA2/PGI2 balance increasing CV risk- Nonselective NSAIDs with high COX2 inhibition seem to have higher cardiovascular risk- Also increase risk of fluid retention and edema