Download
1 / 57
580 likes | 745 Views
Ionic and Ceramic Compounds & Polymers. Materials for Biological Applications. Hydroxyapatite. Chemical formula Ca10(PO4)6(OH)2 Background

E N D
Ionic and Ceramic Compounds &Polymers Materials for Biological Applications
Hydroxyapatite • Chemical formula • Ca10(PO4)6(OH)2 • Background • Hydroxyapatite is chemically similar to the mineral component of bones and hard tissues in mammals. It is one of few materials that are classed as bioactive, meaning that it will support bone ingrowth and osseointegration when used in orthopaedic, dental and maxillofacial applications. The chemical nature of hydroxyapatite lends itself to substitution, meaning that it is not uncommon for non-stoichiometric hydroxyapatites to exist. The most common substitutions involve carbonate, fluoride and chloride substitutions for hydroxyl groups, while defects can also exist resulting in deficient hydroxyapatites • Key Properties The ability to integrate in bone structures and support bone ingrowth, without breaking down or dissolving (i.e it is bioactive). Hydroxyapatite is a thermally unstable compound, decomposing at temperature from about 800-1200°C depending on its stoichiometry. Generally speaking dense hydroxyapatite does not have the mechanical strength to enable it to succeed in long term load bearing applications.
Applications • Bioceramic Coatings • Coatings of hydroxyapatite are often applied to metallic implants (most commonly titanium/titanium alloys and stainless steels) to alter the surface properties. In this manner the body sees hydroxyapatite-type material which it is happy to accept. Without the coating the body would see a foreign body and work in such a way as to isolate it from surrounding tissues. To date, the only commercially accepted method of applying hydroxyapatite coatings to metallic implants is plasma spraying. • Bone Fillers Hydroxyapatite may be employed in forms such as powders, porous blocks or beads to fill bone defects or voids. These may arise when large sections of bone have had to be removed (e.g. bone cancers) or when bone augmentations are required (e.g maxillofacial reconstructions or dental applications). The bone filler will provide a scaffold and encourage the rapid filling of the void by naturally forming bone and provides an alternative to bone grafts. It will also become part of the bone structure and will reduce healing times compared to the situation, if no bone filler was used.
CERAMIC BONDING • Bonding: --Mostly ionic, some covalent. --% ionic character increases with difference in electronegativity. • Large vs small ionic bond character: 14
IONIC BONDING & STRUCTURE • Charge Neutrality: --Net charge in the structure should be zero. --General form: • Stable structures: --maximize the # of nearest oppositely charged neighbors. 15
AmXp STRUCTURES • Consider CaF2 : • Based on this ratio, coord # = 8 and structure = CsCl. • Result: CsCl structure w/only half the cation sites occupied. • Only half the cation sites are occupied since #Ca2+ ions = 1/2 # F- ions. 18
STRUCTURE OF COMPOUNDS: NaCl • Compounds: Often have similar close-packed structures. • Structure of NaCl • Close-packed directions --along cube edges. 21
Diamond, BeO and GaAs are examples of FCC structures with two atoms per lattice point
MATERIALS AND PACKING Crystalline materials... • atoms pack in periodic, 3D arrays • typical of: -metals -many ceramics -some polymers crystalline SiO2 Noncrystalline materials... • atoms have no periodic packing • occurs for: -complex structures -rapid cooling "Amorphous" = Noncrystalline noncrystalline SiO2 26
GLASS STRUCTURE • Basic Unit: • Glass is amorphous • Amorphous structure occurs by adding impurities (Na+,Mg2+,Ca2+, Al3+) • Impurities: interfere with formation of crystalline structure. • Quartz is crystalline SiO2: (soda glass) 28
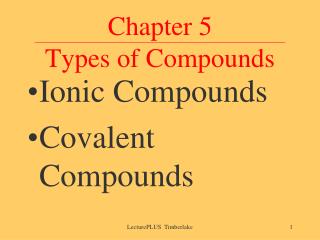
The crystal structure of graphite. Graphite is composed of planes of hexagonally arranged, covalently bonded carbon atoms. The parallel planes are held in place by van der Waals bonds.
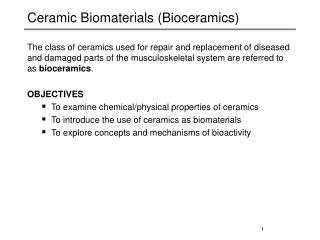
The structure of single-walled carbon nanotubes (SWNTs). (a) the sheets of graphite represented in this figure could be visualized to form a SWNT by rolling one side of the sheet to contact with the other. The twist, or chirality, of the SWNT is defined by a two-dimensional vector, Ch. Two special cases of SWNT are the zigzag (m=0) and armchair (m=n) conformations. These terms refer to the pattern of carbon atoms that one would see along the Ch vector. (b) The 3D structure of a carbon nanotube.
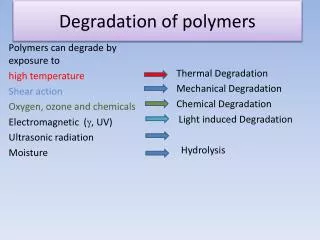
Defects Schottky defects in ceramic crystals. Defects have to occur in pairs to maintain charge neutrality.
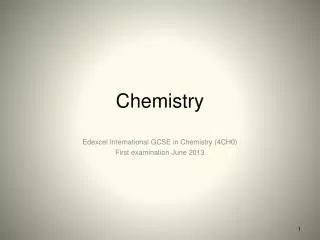
Defects Frenkel defects in ceramic crystals. This usually only occurs with cations, as anions are too large to form an interstitial pair.
POLMER MICROSTRUCTURE • Polymer = many mers Adapted from Fig. 14.2, Callister 6e. • Covalent chain configurations and strength: Direction of increasing strength Adapted from Fig. 14.7, Callister 6e. 2
THERMOPLASTICS VS THERMOSETS • Thermoplastics: --little cross linking --ductile --soften w/heating --polyethylene (#2) polypropylene (#5) polycarbonate polystyrene (#6) • Thermosets: --large cross linking (10 to 50% of mers) --hard and brittle --do NOT soften w/heating --vulcanized rubber, epoxies, polyester resin, phenolic resin 3
MOLECULAR WEIGHT & CRYSTALLINITY • Molecular weight, Mw: Mass of a mole of chains. • Tensile strength (TS): --often increases with Mw. --Why? Longer chains are entangled (anchored) better. • % Crystallinity: % of material that is crystalline. --TS and E often increase with % crystallinity. --Annealing causes crystalline regions to grow. % crystallinity increases. 4
At right, the common mer elements. Mer weights are calculated by the number of each element times its molecular weight. For example, polytetrafluoroethylene is: 2(carbon)*12.011g/mol * 4(flourine)*19.00 g/mol = 100.022 g/mol
Number average and weight average molecular weight, Mn and Mw Number average and weight average degree of polymerization, nn and nw
Conformations of polymers. Single macromolecules can take a variety of shapes, primarily due to the rotation of the carbon atoms in the backbone. Polymer configurations with a C=C double bond (polyisoprene). (a) the “cis” configuration: CH3 and H constituents are found on the same side of the C=C double bond (cis-isoprene is a natural rubber) (b) Trans configuration: CH3 and H are on opposite sides of the double bond
Depiction of a typical conformation for a polymer molecule. Note the large number of bends and kinks present. These types of molecular entanglements play a large role in the mechanical properties of polymers. The end-to-end distance of the polymer chain is denoted by “r”.
Common polymer configurations (“R” group represents a generic side group or atom). • Isotatic configuration: R groups are arranged on the same side of the chain. • Syndiotactic configuration: R groups alternate from side to side • Atactic configuration: R groups are situated randomly. • In this figure, the solid extensions are oriented out of the page and the dashed are into the page.
Overall structures of polymers. • Linear polymers have their repeat units joined end-to end • Branched polymers are formed by synthesis that encourages formation of chains that branch off from main polymer chain • Crosslinked polymers possess adjacent chains that are joined at certain points via covalent bonds, forming a three-dimensional network • Network polymers have tri- or multifunctional mer units that can bind monomers or other polymers to produce three-dimensional network structures.
Types of copolymers: • Random copolymer – the two mer units are distributed along the chain with no pattern • Alternating copolymer – mer types alternate • Block copolymer – each type of repeat unit is clustered in regions (blocks) along the chain • Graft copolymer – homopolymer chains are attached to a main homopolymer chain containing a different repeat unit
Joint Replacement • Joint replacement (arthroplasty) is usually conducted to relieve arthritis pain or fix severe physical joint damage.
History • The earliest recorded attempts to replace hips were carried out in Germany ~1891, using an ivory ball to replace the femoral head (the ball on the femur). • In 1925, a surgeon in Boston, Massachusetts, M.N. Smith-Petersen, M.D., molded a piece of glass into the shape of a hollow hemisphere which could fit over the ball of the hip joint and provide a new smooth surface for movement. While proving biocompatible, the glass could not withstand the stress of walking and quickly failed. Other materials for "mold arthroplasty" were tried, including plastic and stainless steel. Stainless steel was used to resist corrosion by During the 1940's, mold arthroplasty was "state of the art."
A dramatic improvement was made in 1936 when scientists manufactured a cobalt-chromium alloy which was almost immediately applied to orthopaedics. This new alloy was both very strong and resistant to corrosion, and has continued to be employed in various prostheses since that time. While this new metal proved to be a great success, the actual resurfacing technique was found to be less than adequate. It became clear that pain relief was not as predictable as hoped, and hip movement remained limited for many patients. Mold arthroplasty also did not allow surgeons to treat the numerous and varied arthritic deformities of the hip. The search for different types of prostheses continued.
1950s: The prosthesis consisting of a metal stem which was placed into the marrow cavity of the femur, connected in one piece with a metal ball which fit into the hip socket was employed • . While very popular in the 1950's, results remained unpredictable and arthritic destruction of the socket persisted. • No truly effective method of securing the component to the bone. Large numbers of patients developed pain because of this loosening of the implant. The desired result was still not achieved.
Polymer materials were introduced as rubbing surfaces: • As early as 1938, Dr. Jean Judet and his brother, Dr. Robert Judet, of Paris, attempted to use an acrylic material to replace arthritic hip surfaces. This acrylic provided a smooth surface, but unfortunately tended to come loose. • Charnley (England, 1958) addressed the eroded arthritic socket by replacing it with a Teflon implant. He hoped this would allow for a smooth joint surface to articulate with the metal ball component. When the Teflon did not achieve this goal, he went on to try polyethylene. This worked wonderfully well. In order to obtain fixation of this polyethylene socket as well as the femoral implant to the bone, Charnley borrowed polymehtylmethacrylate from the dentists. this substance, known as bone cement, was mixed during the operation then used as a strong grouting agent to firmly secure the artificial joint to the bone. Truly this was the birth of "total hip replacement."
In 1960 Dr. San Baw, a Burmese orthopaedic surgeon, pioneered the use of ivory hip prostheses to replace ununited fractures of the neck of femur ("hip bones"), when he first used an ivory prosthesis to replace the fractured hip bone of an 83 year old nun. An 88% success rate was shown in patients ranging from the ages of 24 to 87, who were able to walk, squat, ride the bicycle and play football (soccer) a few weeks after their fractured hip bones were replaced with ivory prostheses. Ivory may have been used because it was cheaper than metal at that time in Burma and also was thought to have good biomechanical properties including "biological bonding" of ivory with the human tissues nearby. • With modern hip replacement surgery, one can expect to walk, using a cane for balance, within a week.
Hip Replacement Demographics • Between 200,000 and 300,000 hip replacement operations are performed in the United States each year, most of them in patients over the age of 60. • Only 5–10% of total hip replacements as of 2002 were in patients younger than 50. • Reasons for concentration in older adults: • Arthritis and other degenerative joint disorders are the most common health problems requiring hip replacement, and they become more severe as people grow older. • The limited life expectancy of the prostheses used in hip replacements. Because THR is a complex procedure and requires a long period of recovery after surgery, doctors generally advise patients to put off the operation as long as possible so that they will not need to undergo a second operation later to insert a new prosthesis. • This demographic picture is changing rapidly, however, because of advances in designing hip prostheses, as well as changes in older Americans' rising expectations of quality of life. In addition, hip prostheses are lasting longer than those used in the 1960s; one study found that 65% of the prostheses in patients who had had THR before the age of 50 were still intact and functioning well 25 years after the surgery. A larger number of hip replacements are now being done in younger patients, and the operation itself is being performed more often. One expert estimates that the annual number of hip replacements in the United States will rise to 600,000 by 2015. • Average Cost for Total Hip Replacement: $80,000. Surgery costs vary from country to country, with the US typically being among the highest-priced markets, and countries like Thailand, Cuba and Argentina, among the lowest.
Statistics about Knee and Hip Replacement Surgery The upward trends in the utilization of total hip and knee replacement between 1969 and 2003 detail the national need for these procedures. • · The age and gender-adjusted incidence per 100,000 person-years significantly increased from 1971 to 2003, representing a greater than 400% increase in the incidence of total knee replacement (as compared with a 55% increase in total hip replacement during the same period). • · There was a significantly higher utilization rate for women. • · The incidence increased with the patient's age for total knee replacement, except in patients more than eighty years old. • · The largest percentage increase was in patients less than fifty years old. • · There was a significant increase in the proportion of total knee replacements performed for the treatment of osteoarthritis, from 51% during 1971-1975 to 92% in 2000- 2003. • · · It is projected that the number of primary total knee replacements will increase from 450,400 to 3.48 million by 2030, compared with a growth in the number of primary total hip replacements from 208,600 to 572,100 during the same interval. • · The volume of revision total hip replacements is projected to grow from 40,800 in 2005 to 96,700 in 2030 (a 137% increase). • · The volume of revision total knee replacements is projected to grow from 38,300 in 2005 to 268, 200 in 2030 (a 600% increase).
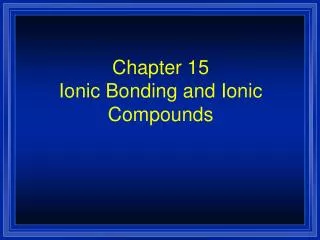
In this X-ray, the patient’s right hip (left of image) has been replaced, with the “ball” of this ball-and-socket joint replaced by a metal head that is set in the thighbone or femur and the socket replaced by a white plastic cup (clear in this X-ray). Pelvic anatomy consistent with that of a female (large infrapubic angle, large pelvic opening).
Modern Artificial Hip Joints The modern artificial joint utilize: • a metal (originally stainless steel) femoral component, • a teflon acetabular component which was replaced by Ultra High Molecular Weight Polyethylene or UHMWPE in 1962, both of which were fixed to the bone using • PMMA (acrylic) bone cement, and/or screws. • Lubricated with synovial fluid (a thick, stringy fluid naturally occurring in joints) • Small femoral head reduces wear rate, but is less stable. Large head is less likely to dislocate, but produces more wear debris due to increased surface area. • Recently the use of a polished tapered cemented hip replacement and uncemented hip replacements have become more popular. • 200,000 – 300,000 hip replacements performed each year in the U.S.
Complications • Infection • Recurrent dislocation • These two complications occur in about 1% of cases • In the long term, many problems relate to osteolysis from wear debris. (The active resorption or dissolution of bone tissue as part of an ongoing disease process) An inflammatory process causes bone resorption and subsequent loosening or fracture often requiring revision surgery • Chronic pain (often caused by nerve damage during surgery)
Knees • First attempts at knee replacements in 1950s. The first knee replacements had "astronomical" failure rates. The knee rotates in more directions than the hip, and the artificial joint needs to be more complicated. • Hinges led to inflammation, pain and loosening and were unreliable in the mid 1960s • Modern knee arthroplasty began in late 60s with a metal on plastic knee replacement secured to the bone with cement. • Today with metal backing of the plastic components, an increased inventory of appropriate sizes of implants, and markedly better instruments to perform the procedure, knee replacement results have equaled or surpassed those of hip replacement. • Since the first knee replacements in the 70s, the joint has been redesigned to mimic the real joint, and now success rates are similar to those for hips. • Approximately 150,000 knee replacements are performed annually in the United States.
Modern Knee Replacements • Hinged knee designs are “constrained” Due to the problems of constrained components, new designs are semi-constrained. In the early 1970s a design know as a total condylar implant was introduced. The shape of the tibial component was such as to mimic the stabilizing influence of the ligaments, though there was no hinge connection between femur and tibia. The majority of designs today are of this type. • Knee replacement components can be fixed to bone either with or without cement. The cement used is normally a material called polymethylmethacrylate (PMMA) and is identical to that used at cemented hip replacement. It may also contain impregnated antibiotic in order to minimize the chances of infection creeping in at surgery. Cementless components are normally coated with small beads, or irregularities, sometimes special chemicals, to encourage the patient's bone to grow into the component, thereby securing the artificial knee. Commonly the metal used for the femoral and tibial components is cobalt-chrome with a high-density polyethylene (HDPE) spacer used between the two to allow a low friction articulation.
Shoulder Joint Replacement The first recorded attempt of shoulder joint replacement occurred in 1892 in a patient suffering from severe arthritis. The first generation of shoulder implants were the “Monoblock” shoulder implants. These began in 1953 and consisted of a single piece – the head of the humerus could not be moved, and thus rarely “fitted” the patient perfectly. The second generation of shoulder implants, named the “Modular Prosthesis,” had independent segments for the head and stem. These were better adapted to the individual patient anatomies because alternative head and stem parts could be chosen.
The third generation of shoulder implants were called the “Anatomical” generation, because they have increased similarities with the actual anatomical shoulder. These are much more adapted to each individual patient's anatomy and do not hinder the mobility of existing muscles, tendons, and ligaments. • Modern shoulder replacement joints look very similar to the structure of the ball and socket of the actual shoulder. The head and stem provide a new surface for the bones and are either bonded to the existing bone structure within the patient through ingrowth, or by using bone cement.
New Materials • One of the principal reasons for failure of total knee arthroplasty (TKA) is wear the ultra-high molecular weight polyethylene (PE) insert. Attempts to alleviate this problem have focused on highly on improved biomaterials such as highly crosslinked PE, ceramic materials, and alternative metals such as tantalum.
Materials: bearing surfaces • Improved metallurgy and manufacturing have resulted in resurgence of metal-on-metal bearing surfaces • Improved hardness and wear resistance • Improved clearance and conformity of bearing surfaces • Higher strength and toughness than polymers
Metal Degradative concerns • High release of ionic metallic debris • Toxicity: Metal-on-metal bearings are not recommended for patients with poorly functioning kidneys because metal ions excreted through the kidneys can build up in the blood. • osteolysis and implant loosening in total hip patients with metal-on-metal bearings may be associated with hypersensitivity to metallic debris • Surface replacement with metal on metal is a new technology that has gained a great deal of recent interest. Hip surface replacement preserves more bone in the patient than conventional hip replacement. This has the potential of being a first-line treatment of end-stage arthritis in younger, active patients.
Metal on Polyethylene Bearings • The adverse effects of oxidation during radiation sterilization • Polyethylene components, like most medical devices, are sterilized by exposure to gamma radiation. The radiation, while penetrating through the component, has sufficient energy to break the chains that form the molecular backbone of the polymer. If the radiation exposure is performed while the component is exposed to air, the broken ends can react with oxygen, causing harmful changes, including a decrease in molecular weight, a dramatic loss of ductility, and a decrease in strength. The combined effect may make the polyethylene markedly more susceptible to wear.
Approaches to minimize degradation of PE • Placing polyethylene joint replacement components into sealed packages that contain either a vacuum or an inert gas, such as nitrogen or argon, instead of air. • Replacing radiation altogether, instead exposing polyethylene components to ethylene oxide or gas plasma, neither of which imparts sufficient energy to cause oxidation. • Increasing dose of radiation to promote crosslinking of polymer chains • early results show a dramatic decrease in wear of between 30 and 96 percent in total hip replacements over that seen with conventional polyethylene. • Disadvantage: increased crosslinking makes material more brittle
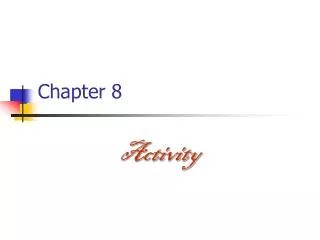
Comparison of volumetric wearrates in pin on discwear test (mm3/million cycles) of different materialscombinations: note that alumina on alumina pairsshow lowest wear rates under laboratory conditions
Ceramic bearings • Advantages • Fully dense ceramics, alumina and zirconia, are used in total joint replacements specifically for the purpose of providing more wear resistant bearing surfaces; they have few other mechanical advantages over metallic alloys. Because of their hardness, ceramics can be polished to a very smooth finish and remain relatively scratch resistant while in use as a bearing surface. • Disadvantages • The most significant disadvantage of ceramics is their brittle nature, making them susceptible to fracture. As with the case of metal-on-metal bearings, where improvements in metallurgy have sparked renewed interest, improvements in ceramic quality have led to increased interest in ceramic bearings. • Patients whose active lifestyles subject them to repetitive impact are not good candidates for ceramic bearings.
Types of Ceramic Bearing Materials • Alumina-on-polyethylene • Long term experience with alumina-on-polyethylene bearings for hip replacement shows reduced wear rates over those typically seen with metal-on-polyethylene bearings, with an associated decrease in osteolysis. • Zirconia-on-polyethylene • The use of zirconia as a bearing surface against polyethylene has not proven as successful clinically as alumina-on-polyethylene bearings. A direct comparison among alumina-, zirconia-, and metal-on-conventional polyethylene bearings in total hip patients revealed the highest wear rate in the zirconia group. • The tendency of zirconia to change its crystalline structure to a form that is less tough, is a disadvantage of this material. The transformation is accompanied by a marked decrease in toughness that makes the material more susceptible to roughening and increased wear. • Alumina-on-Alumina • Used more extensively in Europe than the U.S. • In general, alumina-on-alumina joints have shown very low wear rates clinically, though the results are design dependent. Recent reports also show excellent wear resistance in young patients, with no measurable wear and no evidence of osteolysis even beyond a decade of follow-up. • Very few implant fractures have been observed, even in this high demand patient population, lending further credence to the improved mechanical properties of alumina.