Download
1 / 17
170 likes | 298 Views
Medicaid Coverage Expansion for SUD Services The San Mateo County Experience. April 2013. Overview. Design of LIHP/MCE in SMC Progress in core implementation areas Successes, challenges, lessons Provider Readiness Next Steps. What is “MCE”. MCE = Medicaid Coverage Expansion

E N D
Medicaid Coverage Expansion for SUD ServicesThe San Mateo County Experience April 2013
Overview • Design of LIHP/MCE in SMC • Progress in core implementation areas • Successes, challenges, lessons • Provider Readiness • Next Steps
What is “MCE” • MCE = Medicaid Coverage Expansion • Low income health program for adults who have incomes from 0-133% of the Federal Poverty Level. • MCE is a "bridge" program created by the State of California and the federal government for individuals who are expected to qualify for expanded Medicaid benefits in 2014,under the new federal health care reform law.
Covered Substance Use Services* (San Mateo County’s LIHP/MCE Program) • Assessment • Behavioral Health Integration • Case Management • Collateral Services • Day Care Rehabilitation • Detoxification • Group Counseling • Individual Counseling • Medication Assisted Treatment • Narcotic Replacement Therapy (Methadone) • Outpatient Treatment • Residential Acute Stabilization • Residential Perinatal Treatment • Residential Treatment Including Detoxification • Screening and Intervention *CA Dept of Health Care Services, San Mateo County LIHP Contract, Exhibit A, Attachment 15, 8/18/11
MCE: Year in ReviewCore Implementation Areas • Eligibility and Enrollment • Medical Necessity • Treatment Authorization • Treatment Services • Service Billing • Documentation • Managing the Budget • Reporting • Electronic Health Records Transition
Eligibility & Enrollment • Streamlined health coverage application process for homeless and AOD providers • Successful interagency partnership among HPSM, CHA, HCU, BHRS, and AOD Providers • FY 11/12 • 385 Clients enrolled via AOD provider sites • 70% via AOD Provider-HCU Partnership • 30% via Palm Detox - BHRS Health Insurance Outreach Program Partnership • Unknown # enrolled by CHAs at county clinics
Enrollment & EligibilityChallenges and Lessons • Transitory nature of population • Picture Identification requirements • Failure to disclose all income (ie: unemployment) • Individuals with benefits in neighboring counties • Delayed notification of coverage to providers • No automated “back-end” eligibility verification once billing is submitted
Medical Necessity • Developed by team of BHRS, Providers, and clinical experts • Informed by ASAM, medical necessity requirements of other health insurers. • Provider capacity expansion • Diagnosis - staffing implications and recommend language change to diagnostic impression • Staff Credentialing Requirements (AOD certified vs licensed)
Treatment Authorizations • Prior treatment service authorizations required. • ACCESS Call Center processes MCE Authorization and Re-Authorization Requests, via Avatar • Service Packages, initial authorization period • Residential Detoxification Services– 5 calendar days maximum • Residential Services – 60 calendar day (2 months) maximum • Intensive Outpatient Services – 120 day (4 months) maximum • Outpatient Services– 6 months maximum • Narcotic Replacement Treatment – 1 year maximum • Retroactive “auth” requests permitted when client MCE is “pending enrollment” up to 90 days from date of first service.
MCE Service Billing • $2,894,627 – FY 11/12 billing total • Represents $1,447,313 in new federal funds for SUD treatment in San Mateo County • Limited provider experience tracking and billing for services by the minute (OP only) • Temporary “scantron” was up for billing, until transition to Avatar was completed
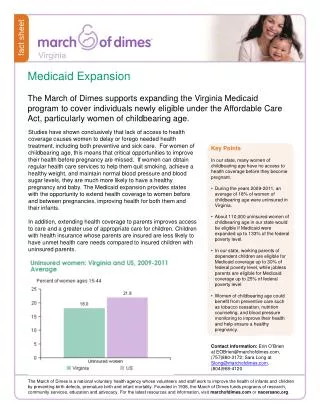
Medicaid Expansion in 2014 • The good news…the Supreme Court upheld the Affordable Care Act. • In 2014, the estimated 20% of uninsured Californians will be able to obtain health coverage via the Exchange or Medicaid expansion. • MCE SUD benefit and provider requirements –still pending State determination • CA considering “State” verses “County” option
SUD Provider Readiness • Changing face of partners and referrals sources, from criminal justice to primary care • Credentialing of staff – State ADP requirements vs. health insurance requirements (licensing); ability to diagnose. • Treatment Program design – care based on individual needs, not on “program design” (ie: 90 day program) • Documentation of medical necessity and services • Knowledge of billing codes • Lack relationships with private insurers, primary care providers.
Next Steps: Primary Care • Navigate the primary care system • Develop relationships • Establish referral & communications protocols (bi-directional) • Provide outreach materials to PCP • Expanding medication assisted treatment • Improve physical and mental health of SUD clients through greater coordination
Thank you! Clara Boyden SMC Behavioral Health & Recovery Services cboyden@smcgov.org 65-802-5101