Download
1 / 1
10 likes | 755 Views
REVERSE TAKOTSUBO CARDIOMYOPATHY IN AN ELDERLY PATIENT WITH BACTEREMIA. Capt Debra Koenigsberger, USAF, MC David Grant Medical Center, Travis AFB, CA. INTRODUCTION. DISCUSSION. Reverse takotsubo cardiomyopathy (RTCM): Subtype of stress cardiomyopathy

E N D
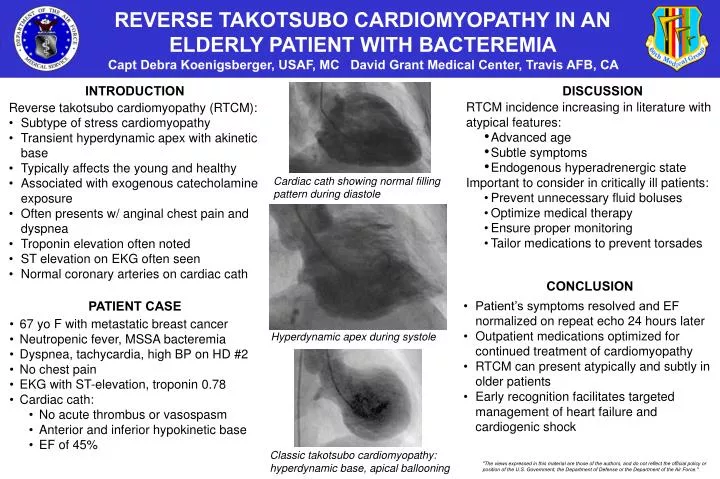
REVERSE TAKOTSUBO CARDIOMYOPATHY IN AN ELDERLY PATIENT WITH BACTEREMIA Capt Debra Koenigsberger, USAF, MC David Grant Medical Center, Travis AFB, CA INTRODUCTION DISCUSSION • Reverse takotsubo cardiomyopathy (RTCM): • Subtype of stress cardiomyopathy • Transient hyperdynamic apex with akinetic base • Typically affects the young and healthy • Associated with exogenous catecholamine exposure • Often presents w/ anginal chest pain and dyspnea • Troponin elevation often noted • ST elevation on EKG often seen • Normal coronary arteries on cardiac cath • RTCM incidence increasing in literature with atypical features: • Advanced age • Subtle symptoms • Endogenous hyperadrenergic state • Important to consider in critically ill patients: • Prevent unnecessary fluid boluses • Optimize medical therapy • Ensure proper monitoring • Tailor medications to prevent torsades Cardiac cath showing normal filling pattern during diastole CONCLUSION PATIENT CASE • Patient’s symptoms resolved and EF normalized on repeat echo 24 hours later • Outpatient medications optimized for continued treatment of cardiomyopathy • RTCM can present atypically and subtly in older patients • Early recognition facilitates targeted management of heart failure and cardiogenic shock • 67 yo F with metastatic breast cancer • Neutropenicfever, MSSA bacteremia • Dyspnea, tachycardia, high BP on HD #2 • No chest pain • EKG with ST-elevation, troponin 0.78 • Cardiac cath: • No acute thrombus or vasospasm • Anterior and inferior hypokinetic base • EF of 45% Hyperdynamic apex during systole Classic takotsubo cardiomyopathy: hyperdynamic base, apical ballooning "The views expressed in this material are those of the authors, and do not reflect the official policy or position of the U.S. Government, the Department of Defense or the Department of the Air Force."