Download
1 / 49
500 likes | 884 Views
Hemophilia: The Royal Disease. Natalia A Palacio April 2006. Definition. Hemophilia- “love of bleeding” 2 types: A and B Hemophilia A: X linked recessive hereditary disorder that is due to defective or deficient factor VIII. History.

E N D
Hemophilia: The Royal Disease Natalia A Palacio April 2006
Definition • Hemophilia- “love of bleeding” • 2 types: A and B • Hemophilia A: X linked recessive hereditary disorder that is due to defective or deficient factor VIII
History • First references are mentioned in Jewish texts in second century AD by Rabbi Ben Gamaliel who correctly deduced that sons of mother- that he did not know at that time- was an hemophilic carrier bled to death after circumcision. Hence he made a ruling that excepted newborn Jewish boys of this ritual if two previous brothers had had bleeding problems with it. • Then Rabbi and physician Maimonides in the XII century noted that the mothers were the carriers, hence the second ruling that if she married twice the newborns from the second marriage were also excepted. • In 1800 John Otto a physician in Philadelphia wrote a description of the disease where he clearly appreciated the cardinal features: an inherited tendency of males to bleed • In 1928 the word Hemophilia was defined.
Incidence • It is the second most common inherited clotting factor abnormality (after von Willebrand disease) • 1 in 5000-10000 live male births • No difference between racial groups
Pathophysiology • Sequential activation of a series of proenzymes or inactive precursor proteins (zymogens) to active enzymes, resulting in significant stepwise response amplification. • Two pathways: intrinsic and extrinsic measured by two lab tests
Pathophysiology • F VIII is a cofactor for intrinsic Xa • FvW is its carrier • Activated by Xa and thrombin • Inactivated by activated protein C in conjunction with protein S
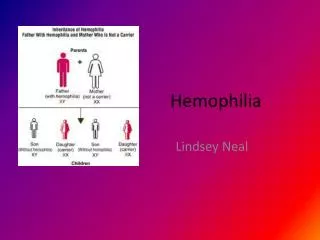
Genetics • Transmitted by females, suffered by males • The female carrier transmits the disorder to half their sons and the carrier state to half her dtrs • The affected male does not transmit the disease to his sons (Y is nl) but all his dtrs are all carriers (transmission of defected X)
Genetics • Hemophilia in females • If a carrier female mates with an affected male there’s the possibility that half their daughters are homozygous for the disease • Other possibility: Turner syndrome (45,X0) with a defective X
Genetics • Factor VIII gene • Xq28 • One of the largest genes known-186k base pairs • 26 exons • Its large size predisposes it to mutations
Genetics • In Hemophilia A there is no uniform abnormality. There are deletions, insertions, and mutations • 200 genes studied-7 dif mutations • 4->transposition of a single base-3 lead to stop codon, 1 changed an aa • 3->deletions • Aprox 40% of severe hemophilia A is caused by a major inversion in the gene- the breakpoint is situated within intron 22
Genetics • In 1/3 of hemophiliac patients, there is no family history of bleeding. This is consistent with the Haldane hypothesis that predicted that maintenance of a consistent frequency of a genetic disorder in the population would require that aprox 1/3 cases are spontaneous mutations
Clinical manifestations • Frequency and severity of bleeding are related to F VIII levels • Coinheritance of prothrombotic mutations (i.e. Factor V Leiden) can decrease the risk of bleeding
Clinical Manifestations:Hemarthrosis • The most common, painful and most physically, economically and psychologically debilitating manifestation. • Clinically: • Aura: tingling warm sensation • Excruciating pain • Generally affects one joint at the time • Most commonly: knee; but there are others as elbows, wrists and ankles. • Edema, erythema, warmth and LOM • If treated early it can subside in 6 to 8 hs and disappear in 12 to 24 hs. • Ddx: DJD • Complications: Chronic involvement with joint deformity complicated by muscle atrophy and soft tissue contractures
Clinical Manifestations:Hemarthrosis • Pathophysiology: • Bleeding probably starts from synovial vessels into the synovial space. • Reabsorption of this blood is often incomplete leading to chronic proliferative synovitis, where the synovium is more thickened and vascular, creating a “target joint” with recurrence of bleeding. • There is destruction of surrounding structures as well-bone necrosis and cyst formations, osteophytes • Terminal stage: Chronic Hemophiliac arthropathy: fibrous or bony ankilosing of the joint.
Clinical Manifestations:Hemarthrosis • There is a radiological classification for the stages
Stage III- early subchondral cyst Clinical ManifestationsHemarthrosis-Images • Stage IV- narrowing of intraarticular space
Clinical ManifestationsHematomas • Subcutaneous and muscular hematomas spread within fascial spaces, dissecting deeper structures • Subcutaneous bleeding spreads in characteristic manner- in the site of origin the tissue is indurated purplish black and when it extends the origin starts to fade • May compress vital structures: such as the airway if it is bleeding into the tongue throat or neck; it can compromise arteries causing gangrene and ischemic contractures are common sequelae, especially of calves and forearms • Muscle hematomas: 1)calf,2)thigh,3)buttocks,4)forearms • Psoas hematoma- if right sided may mimic acute appendicitis • Retroperitoneal hematoma: can dissect through the diaphragm into the chest compromising the airway. It can also compromise the renal function if it compresses the ureter
Clinical manifestationsPseudotumors • Dangerous and rare complication • Blood filled cysts that are gradually expanding • Occur in soft tissues or bones. • Most commonly in the thigh • As they increase in size they erode contiguous structures. • May require radical surgeries or amputation, and surgery is often complicated with infection A pseudotumor is deforming the cortex of the femur (arrow). Other ossified masses in the soft tissues (arrowheads) are probably soft-tissue pseudotumors.
Clinical manifestationsIntracranial hemorrhage • Leading cause of death of hemophiliacs • Spontaneous or following trauma • May be subdural, epidural or intracerebral • Suspect always in hemophilic patient that presents with unusual headache • If suspected- FIRST TREAT, then pursue diagnostic workup • LP only when fVIII has been replaced to more than 50%
Clinical manifestationsOthers • Gastrointestinal Bleeding: PUD is 5 times more common in hemophiliac patients than regular males. Associated with ingestions of NSAIDs for hemarthrosis. Frequent cause of UGIB • Mucous Bleeding: Epistaxis, gum bleeding. • Genitourinary Bleeding: Frequently severe hemophiliac can experience hematuria and a structural lesion should be ruled out.
Laboratory diagnosis • Nomenclature: • FVIII protein that is lacking or aberrant • FVIIIc functional FVIII measured by clotting assays • FVIIIag Antigenic protein that can be detected with immunoassays • Deficit can be quantitative or qualitative • General Lab: prolonged aPTT, nl PT and BT • Mixing studies: aPTT corrects with normal plasma –if there are no factor VIII antibodies present • Clotting assays: F VIII activity, expressed in % of normal DecreasedQUANTITATIVE • Immunoassays: “Cross Reactive Material” Positive- there is an antigen similar to the F VIII protein- QUALITATIVE
Differential Diagnosis • Clinically impossible to differentiate from Hemophilia B- FIX def- Christmas’ disease • Type 2N vWD, transmitted as an autosomal recessive trait, is characterized by mutations in VWF within the factor VIII binding domain. Affected patients present with low levels of factor VIII (usually 5 to 15 percent of normal), because of unimpeded proteolytic cleavage of factor VIII, along with a clinical pattern of bleeding similar to that seen in hemophilia A, rather than that associated with classical vWD Should be suspected in families in which an autosomal recessive (rather than X-linked) inheritance pattern is seen.
Carrier detection and Antenatal diagnosis • Family history: if we follow the inheritance pattern a female is a carrier if she: • Has an hemophilic father • Has two hemophilic sons • Has one hemophilic son and has a family history • Has a son but no family history, there is a 67% chance that she is.
Carrier detection and Antenatal diagnosis • Coagulation based assays: • Generally heterozygous females have <50% f VIII levels but if normal it can’t be excluded • vWF is usually normal or elevated in female carriers, so F VIII:FvW ratio is low which adds sensitivity to these tests • DNA based assays: • Southern blot can detect the inversion in intron 22 • If negative for that, there is the need for DNA sequencing • For prenatal diagnosis: DNA testing on choronic villi samples obtained by biopsy at week 12
TreatmentGeneral Considerations • Hemophilia centers should be available for every patient • Several medical specialists may be a part of the patient's care team: • A hematologist • Hemophilia nurses and social workers • An orthopedic surgeon • A blood laboratory specialist • A family physician or internal medicine specialist • A dentist • A physical medicine and rehabilitation (PMR) therapist • Avoidance of aspirin and NSAIDs if at all possible sometimes it is difficult because of the painful hemarthrosis • No IM injections • Counseling for patient and family, both genetic and psychosocial, encouraging normal socialization
TreatmentFactor replacement Replacement of F VIII is the cardinal step to prevent or reverse acute bleeding episodes • Dosing: Replacement products can be given on the basis of body weight or plasma volume ( aprox 5% of body weight) • 1 U/ml = 100% factor activity • Practically 1 unit of F VIII/kg increases F VIII about 0.02 U/ml • In a severe hemophiliac, to raise F VIII to 100% activity or 1 U/ml, we need 50 U/kg • Redosing is based on half life: 8-12 hs • Monitoring of Factor activity is crucial during therapy
TreatmentFactor replacement • Choice of treatment: is based on • Purity of the factor (how concentrated or “purified” the factor is) • Safety • Cost • Nowadays most used therapies are believed to be effective and relatively safe
TreatmentFactor replacement Sources of F VIII • Plasma • FFP was used as the only replacement therapy until 1960s. • Not really much effective since it could only raise f VIII to 20%, by giving the patient many liters • Usually patients experienced severe volume overload (luckily furosemide was introduced around this time) • Patients used to have to spend most of their time in the hospital
TreatmentFactor replacement • Cryoprecipitate • By mid 1960s Pool et al demonstrated that cold insoluble material obtained from plasma contained high levels of F VIII and fibrinogen, achieving a major advance in hemophilia treatment • 1 unit of FFP prepared by cryoprecipitate contains 50-120 U of VIII • Plasma Derived f VIII prepared by monoclonal antibodies.
TreatmentFactor replacement • Before 1985 all plasma derived products were highly contaminated by blood borne virus such as HIV, HBV and HCV which is now incredibly reduced by the introduction of donor screening and viral inactivation techniques such as pasteurization, solvent detergent treatment and ultrafiltration. • However, there is still some theoretical concern about non lipid coated parvovirus, HAV and prion disease such as Creutzfeld-Jakob
TreatmentFactor replacement • Recombinant F VIII • First generation: derived from hamster cell culture. Contains human albumin for stabilization (possible source of viral contamination) • Second Generation: Mutated F VIII, lacking B domain (no role in clotting) that can be stabilized by sucrose “albumin free” • Porcine F VIII • Useful for hemophiliacs with F VIII inhibitors • It is antigenic, property that limits its use to one treatment course
TreatmentFactor replacement • Target level and duration of treatment: depend of severity and site of bleeding
TreatmentOthers • Fibrin Glue • Contains fibrinogen, thrombin and factor XIII • It’s placed in the site of injury and stabilizes clot • Used in dental procedures and after circumcision • Antifibrinolyitic Agents • Epsilon aminocaproic acid • Inhibit fibrinolysis by inhibiting plasminogen activator • Adjuvant therapy for dental procedures • Contraindicated in hematuria • Desmopressin • Transient increase in F VIII levels in pts with mild hemophilia(2-4 times above baseline) • Mechanism: release from endothelial storage sites • Has spared many hemophiliacs of blood borne products in the 1970s • Repeated administration results in a diminished response- tachyphylaxis • Side effects: hyponatremia, facial flushing and headache
TreatmentGene Therapy • Hemophilia is an ideal disease to target for gene therapy since it is caused by mutations in a single identified gene. • A slight increase in factor activity can make a severe hemophilic in mild. • Tight regulation of gene expression is not essential. • Many animal models trials have been studied, being the main problems encountered: immunogenicity and short gene expression. • To date 3 hemophilia A trials in human (aprox 20 patients): transient increase of factor VIII activity and good safety profile. • Main issue remains: finding of a gene delivery system which is nonimmunogenic so as to allow for long term expression.
Course and prognosis • When FVIII concentrate emerged in 1960s, the morbidity and mortality from bleeding in hemophilia decreased • Unfortunately, between 1978-1985 the AIDS crisis hit the hemophiliac community • AIDS still remain the leading cause of death in older hemophiliacs • Patients treated after 1985 should expect to have virtually normal life spans free of the complications of HIV and hepatitis
Course and prognosis • Replacement therapy has its complications and includes: • Development of F VIII antibodies • Liver disease resulting from hepatitis B and C • Infection with HIV
Course and prognosisDevelopment of Antibodies • Specific inhibitor antibodies that neutralize FVIII activity • Most frequently in severe affected patients- affecting 25% • Predisposing factors: severe disease, type of genetic mutation (inversion, nonsense mutation, deletions), family history of inhibitors development • Alloantibody-IgG4- against C2 domain of F VIII protein which interacts with other cascade cofactors (phospholipids) • Seen aprox 9-11 days post factor VIII exposure • Diagnosis: mixing study does not correct aPTT. Bethesda assay: which consists of serial dilutions of plasma is pooled with normal plasma and incubated for 2 hs, then the activity level is measured by coagulation assays. The higher inhibitor titer, the greater the dilution required to demonstrate residual FVIII activity. It is expressed on Bethesda Units: High responders: >5 Bethesda units, low responders <5.
Course and prognosisDevelopment of Antibodies • Treatment: of active bleeding and inhibitor ablation via immune tolerance induction. • High purity FVIII: treatment of life threatening hemorrhages in pts that are low responders • Porcine FVIII: high responders with high inhibitors levels that have life threatening hemorrhages • Prothrombin complex concentrates and activated prothrombin complex concentrates: bypassing agents for thrombosis (prothrombin, fVII, fIX, f X and Prot S and C). Carries high risk of thrombosis and it is difficult to monitor. • rFVIIa: Effective response in 90% of patients. Gets activated by tissue factor, so thrombosis response is more modulated than that of APCCs, however there are no studies comparing them both
Course and prognosisDevelopment of Antibodies • Immunotolerance Induction: process by which a pt is made tolerant to FVIII by repeated daily exposure • Aprox 70% success rate • Eligible pts: severe hemophiliacs with F VIII inhibitors<12 months with a peak of no more than 200 BU/ml. • The sooner initiated, the better
Course and prognosisHepatitis and HIV • Almost all multitransfused patients before 1985 were affected with one or more agents of chronic hepatitis • Around 50% can be expected to develop chronic hepatitis that may lead to cirrhosis • Hepatic injury is worse with coinfection with HIV – there is a five to sixfold increase in end stage liver disease which is not uncommon. • Currently about 80% of older severe hemophiliacs are HIV positive • As of 1985, rigid donor testing and availability of recombinant products has greatly diminished viral transmission.
TreatmentProphylaxis • Prophylactic treatment should be considered in all patients with severe hemophilia • In 1997 was recommended by the Medical and Scientific Advisory Council of the National Hemophilia Foundation. • Candidate should be reliable to manage a central venous catheter device • Administration is three times a week to make a severe hemophiliac a moderate phenotype • There is significant improvement in the clinical condition and quality of life.
HistoryWhy the Royal disease? • This is because Queen Victoria, Queen of England from 1837 to 1901, was a carrier. • Most likely a spontaneous mutation since the duke of Kent (her father) was not affected and her mother did not have any affected children from the previous marriage. • Her eighth child, Leopold, had hemophilia and suffered from frequent hemorrhages. These were reported in the British Medical Journal in 1868. • Leopold died of a brain hemorrhage at the age of 31, but not before he had children. His daughter, Alice, was a carrier and her son, Viscount Trematon, also died of a brain hemorrhage in 1928. • The British family descends from Victoria’s first child Edward who was not affected. Hence this house is disease free.
HistoryWhy the Royal disease? • Beatrice, Victoria’s youngest child had two hemophilic sons and a daughter- Victoria Eugene that was a carrier • She introduced the hemophilia gene into the Spanish royal family by marrying king Alfonso XIII. • By this time, Queen Victoria’s blood was recognized as “defective” and the king may have been warned about Eugene’s carrier state. However, Royalty was more important than X chromosomes.
HistoryWhy the Royal disease? • Alexandra, Queen Victoria's granddaughter, married Nicholas, the Tsar of Russia in the early 1900's. • Alexandra, the Tsarina, was a carrier of hemophilia and her first son, the Tsarevich Alexei, was an hemophiliac • The monk Rasputin gained great influence in the Russian court, partly because he was the only one able to help the young Tsarevich. He used hypnosis to relieve Alexei's pain. • It is speculated that the illness of the heir to the throne, the strain it placed on the Royal family, and the influence of the corrupt and alcoholic monk Rasputin were all factors leading to the Russian Revolution of 1917.
HistoryQueen Victoria’s pedigree Russian House Spanish House British House
But wait….. Which Hemophilia was it A or B???? EITHER!
References • National heart lung blood institute www.nhlbi.nih.gov • www.uptodate.com • Goldman: Cecil textbook of medicine,22nd edition, 1070-1074. • Kessler. New Perspectives in Hemophilia Treatment. Hematology2005; 429-435 • Manucci et al. The hemophilias-from royal genes to gene therapy. NEJM; 2001; 344(23) • Rick M, Walsh C. Congenital bleeding disorders. Hematology 2003; 559-574 • Hoffman: Hematology basic principles and practice, 4th edition. 2017-2026. • National Hemophilia Foundation www.hemophilia.org • Benter E, Coller B et al. Williams Hematology, 6th edition. 1639-1652. 2001 • Greer et al. Wintrobe’s Clinical Hematology, 11th edition.2003