Download

1 / 21
240 likes | 551 Views
External Pacemakers. Rafael Ortega, MD Boston University Medical Center. From the Trenches. 70-year-old woman Returns to OR for expanding neck hematoma Cardiac arrest after intubation Management. OBJECTIVES. Review External Pacemakers (EP) Summarize EP historical evolution

E N D
External Pacemakers Rafael Ortega, MD Boston University Medical Center
From the Trenches • 70-year-old woman • Returns to OR for expanding neck hematoma • Cardiac arrest after intubation • Management
OBJECTIVES • Review External Pacemakers (EP) • Summarize EP historical evolution • Clarify EP indications • Explain the Philips/Agilent HeartStart Unit
3 in 1 Biphasic Unit Manual Defibrillator Automatic Defibrillator External Pacemaker
Question What is “Biphasic”?
A Few Words on “Biphasic” • Biphasic energy is delivered in two directions • Require less energy for defibrillation • Less myocardial injury and myocardial dysfunction • 150 J should be used for defibrillating ventricular fibrillation (in adults)
Waveform Comparison • Monophasic • Biphasic
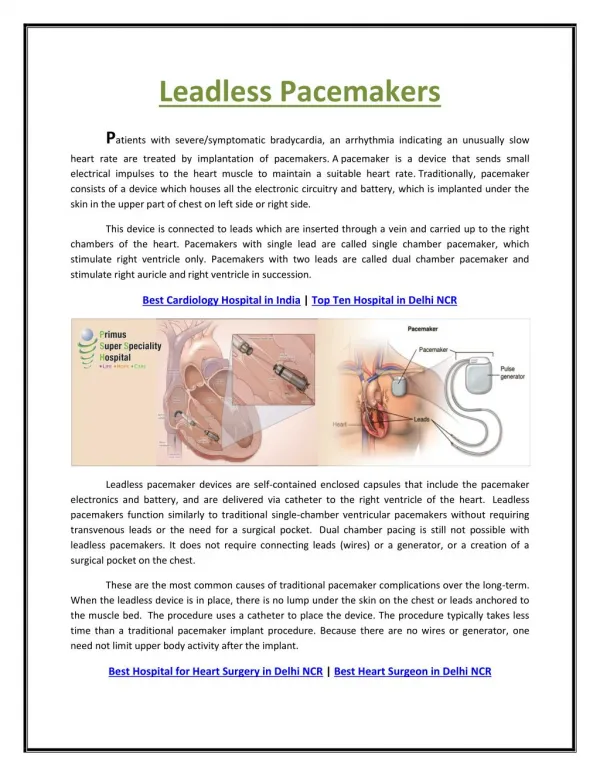
Indications for EP • Temporizing measure in patients with symptomatic bradycardia • Little benefit in pulseless situations • May be useful for overdrive-pacing in certain tachycardias.
Early History • 1791: Galvani electrically stimulates dead frog’s heart • 1872: Duchenne resuscitates child tapping precordium with an electrode • 1932: Hyman designs external pulse generator: "artificial cardiac pacemaker“ • 1952: Zoll uses simultaneous precordial and transesophageal electrodes for pacing
46 Years later • Hesselvik JF. Ortega RA. Simultaneous transesophageal atrial pacing and transesophageal echocardiography in cardiac surgical patients.Journal of Cardiothoracic & Vascular Anesthesia. 12(3):281-3, 1998 Jun.
Who was Dr. Zoll? • A Boston native • Harvard Medical School • Internship BI Hospital • In 1939 joins a research group at BI • WW-ll on Dwight Harken's surgical team Paul Zoll Professor Emeritus HMS
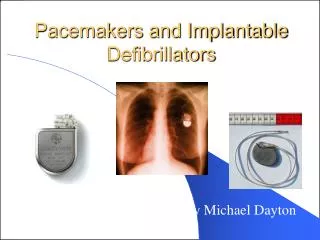
Transvenous Pacing Effect • Temporary and permanent implantable transvenous pacemakers (late 1950’s) superseded the use of external models. • But, these took time to insert • There was still a need for external pacing
1981: A New Era • Zoll patents and introduces a transcutaneous external pacemaker • Longer pulse duration and larger electrode surface • Reduced current required for capture and increased comfort for the patient • New model could be applied much more rapidly
Pulse Duration and Current • Early models used short (1-2 msec) impulses resembling the action potential of skeletal muscles • Zoll increased duration to 4 msec with a 3-fold reduction in threshold • Stimulation 20% over threshold stimulates only the ventricles. • External pacing requires 30-100 times greater current than transvenous pacing
Question What is the effect of EP on hemodynamics?
Hemodynamics • EP can simultaneously stimulate all 4 heart chambers (in dogs) • Madsen echo demonstrated that atrial stimulation was retrograde without opening the mitral valve. • Atrial-pacing threshold in humans is much higher than for ventricles • Net result: loss of the “atrial kick” • Cardiac output is reduced
Reducing Discomfort • Not a problem under GA • If awake, place electrodes in the midline chest and just below the left scapula • Considered sedation
Question Can you perform CPR and use EP at the same time?
EP During CPR • CPR can be performed with EP pads in place. • No electrical hazard to the person performing CPR • However, turning the unit off during CPR is advisable.
No Heart Damage • No enzymatic, EKG, or microscopic evidence of myocardial damage has been found after pacing (dogs and humans) for as long as 60 minutes • Low risk of triggering ventricular fibrillation