Download
1 / 92
930 likes | 1.28k Views
Pacemakers and Internal Cardiac Defibrillators. Mark Wahba Resident Rounds September 11, 2003. See: Brady’s, Blocks, & Pacers. Moritz Haager 1 hr rounds July 17, 2002. Brief History. First described in 1952 Introduced into clinical practice in 1960

E N D
Pacemakers and Internal Cardiac Defibrillators Mark Wahba Resident Rounds September 11, 2003
See:Brady’s, Blocks, & Pacers Moritz Haager 1 hr rounds July 17, 2002
Brief History • First described in 1952 • Introduced into clinical practice in 1960 • First endocardial defibrillators in 1980 • 1991 in USA 1 million people had permanent pacemakers
Outline • Indications • Basics, Pacemaker Components and Code • Complications of Implantation • Pacemaker Malfunction • Management • Disposition • ICD • Guest
Basically: Device that provides electrical stimulation to cause cardiac contraction when intrinsic cardiac electrical activity is slow or absent • http://www.emedicine.com/emerg/topic805.htm
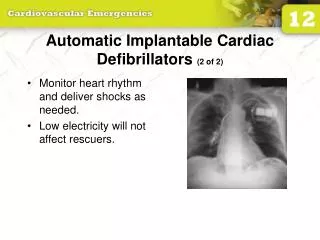
Pacemaker Functions • Stimulate cardiac depolarization • Sense intrinsic cardiac function • Respond to increased metabolic demand by providing rate responsive pacing • Provide diagnostic information stored by the pacemaker
Indications for Pacer • 30 AVB and any of: • Symptomatic bradycardia • Asystole >3 sec or vent escape <40bpm • Post-AVN ablation • Post-op and not expected to improve • Neuromuscular disease • 20 AVB + symptomatic bradycardia • Chronic bi-/trifasicular block w/ intermittent 30 AVB or 20 AVB Type II • Post-MI and any of: • Persistent 20 AVB or 30 AVB • Transient 20 AVB or 30 AVB and BBB • SAN dysfunction + symptomatic brady’s (e.g. SSS) • Recurrent syncope due to carotid sinus stimulation
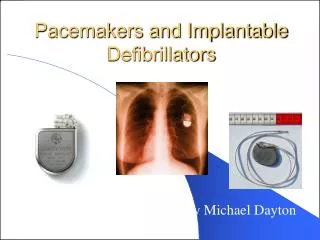
Pacemaker Components • Pulse Generator • Electronic Circuitry • Lead System
Pulse Generator • Subcutaneous or submuscular • Lithium battery • 4-10 years lifespan • long life and gradual decrease in power sudden pulse generator failure is an unlikely cause of pacemaker malfunction
Electronic Circuitry • Sensing circuit • Timing circuit • Output circuit
Bipolar Lead has both negative, (Cathode) distal and positive, (Anode) proximal electrodes Separated by 1 cm Larger diameter: more prone to fracture Compatible with ICD Unipolar Negative (Cathode) electrode in contact with heart Positive (Anode) electrode: metal casing of pulse generator Prone to oversensing Not compatible with ICD Lead System
Difference on an ECG? Bipolar • current travels only a short distance between electrodes • small pacing spike: <5mm + Anode - Cathode
Difference on an ECG? Unipolar • current travels a longer distance between electrodes • larger pacing spike: >20mm + Anode - Cathode
I II III IV V Programmable Antitachy Chamber Chamber Response Paced Sensed to Sensing Functions/Rate Function(s) Modulation Pacemaker Code P: Simple programmable V: Ventricle V: Ventricle T: Triggered P: Pace M: Multi- programmable A: Atrium A: Atrium I: Inhibited S: Shock D: Dual (A+V) D: Dual (T+I) D: Dual (P+S) D: Dual (A+V) C: Communicating O: None O: None O: None O: None R: Rate modulating S: Single (A or V) S: Single (A or V) O: None
Common Pacemakers • VVI • Ventricular Pacing : Ventricular sensing; intrinsic QRS Inhibits pacer discharge • VVIR • As above + has biosensor to provide Rate-responsiveness • DDD • Paces + Senses both atrium + ventricle, intrinsic cardiac activity inhibits pacer d/c, no activity: trigger d/c • DDDR • As above but adds rate responsiveness to allow for exercise
Rate Responsive Pacing • When the need for oxygenated blood increases, the pacemaker ensures that the heart rate increases to provide additional cardiac output Adjusting Heart Rate to Activity Normal Heart Rate Rate Responsive Pacing Fixed-Rate Pacing Daily Activities
Determining type of pacemaker • Wallet card: 5 letter code • CXR: code visible • Single lead in ventricle: VVI • Separate leads DDD or DVI
Single Chamber • VVI - lead lies in right ventricle • Independent of atrial activity • Use in AV conduction disease
Paced Rhythm Recognition VVI / 60
Dual Chamber • Typically in pts with nonfibrillating atria and intact AV conduction • Native P, paced P, native QRS, paced QRS • ECG may be interpreted as malfunction when none is present • May have fusion beats
AP AP VP VP Four “Faces” of Dual Chamber Pacing • Atrial Pace, Ventricular Pace (AP/VP) AV V-A AV V-A Rate = 60 bpm / 1000 ms A-A = 1000 ms
AV V-A AV V-A AP AP VS VS Four “Faces” of Dual Chamber Pacing • Atrial Pace, Ventricular Sense (AP/VS) Rate = 60 ppm / 1000 ms A-A = 1000 ms
V-A AV V-A AV Four “Faces” of Dual Chamber Pacing • Atrial Sense, Ventricular Pace (AS/ VP) AS AS VP VP Rate (sinus driven) = 70 bpm / 857 ms A-A = 857 ms
AV V-A AV V-A AS AS VS VS Four “Faces” of Dual Chamber Pacing • Atrial Sense, Ventricular Sense (AS/VS) Rate (sinus driven) = 70 bpm / 857 ms Spontaneous conduction at 150 ms A-A = 857 ms
Pacemaker Interventions • Magnet application • No universal function of magnet • Model-specific magnet, some activate reed switch asynchronous pacing at pre-set rate • Interrogation / Programming • Model-specific pacemaker programmer can non-invasively obtain data on function and reset parameters
Complications of Pacemaker Implantation • Venous access • Infection • Thrombophelbitis • Pacemaker Syndrome
Venous Access • Bleeding • Pneumo / hemothorax • Air embolism
Infection • 2% for wound and ‘pocket’ infection • 1% for bacteremia with sepsis • S. aureus and S. epidermidis • If bacteremic: start Vancomycin, remove system, TV pacemaker and IV abx for 4-6 weeks, new system
Thrombophlebitis • Incidence 30-50% • 1/3 have complete venous obstruction • b/c of collateralization only 0.5-3.5% devp symptoms • Swelling, pain, venous engorgement • Heparin, lifetime warfarin
Pacemaker Syndrome • Presents w/ worsening of original Sx post-implant of single chamber pacer • AV asynchrony retrograde VA conduction atrial contraction against closed MV + TV jugular venous distention + atrial dilation sx of CHF and reflex vasodepressor effects • Dx of exclusion • Tx w/ dual chamber pacer
4 broad categories • Failure to Output • Failure to Capture • Inappropriate sensing: under or over • Inappropriate pacemaker rate
Failure to Output absence of pacemaker spikes despite indication to pace • dead battery • fracture of pacemaker lead • disconnection of lead from pulse generator unit • Oversensing • Cross-talk: atrial output sensed by vent lead
No Output • Pacemaker artifacts do not appear on the ECG; rate is less than the lower rate Pacing output delivered; no evidence of pacing spike is seen
Failure to capture spikes not followed by a stimulus-induced complex • change in endocardium: ischemia, infarction, hyperkalemia, class III antiarrhythmics (amiodarone, bertylium)
Inappropriate sensing: Undersensing Pacemaker incorrectly misses an intrinsic deoplarization paces despite intrinsic activity • Appearance of pacemaker spikes occurring earlier than the programmed rate: “overpacing” • may or may not be followed by paced complex: depends on timing with respect to refractory period • AMI, progressive fibrosis, lead displacement, fracture, poor contact with endocardium
Undersensing • Pacemaker does not “see” the intrinsic beat, and therefore does not respond appropriately Scheduled pace delivered Intrinsic beat not sensed VVI / 60
Undersensing • An intrinsic depolarization that is present, yet not seen or sensed by the pacemaker P-wavenot sensed Atrial Undersensing
Inappropriate sensing: Oversensing Detection of electrical activity not of cardiac origin inhibition of pacing activity • “underpacing” • pectoralis major: myopotentials oversensed • Electrocautery • MRI: alters pacemaker circuitry and results in fixed-rate or asynchronous pacing • Cellular phone: pacemaker inhibition, asynchronous pacing
VVI / 60 Oversensing • An electrical signal other than the intended P or R wave is detected ...though no activity is present Marker channel shows intrinsic activity...
Inappropriate Pacemaker Rate • Rare reentrant tachycardia seen w/ dual chamber pacers • Premature atrial or vent contraction sensed by atrial lead triggers vent contraction retrograde VA conduction sensed by atrial lead triggers vent contraction etc etc etc • Tx: Magnet application: fixed rate, terminates tachyarrthymia, • reprogram to decrease atrial sensing
Causes of Pacemaker Malfunction • Circuitry or power source of pulse generator • Pacemaker leads • Interface between pacing electrode and myocardium • Environmental factors interfering with normal function
Pulse Generator • Loose connections • Similar to lead fracture • Intermittent failure to sense or pace • Migration • Dissects along pectoral fascial plane • Failure to pace • Twiddlers syndrome • Manipulation lead dislodgement