Download
1 / 30
310 likes | 489 Views
Stem and Progenitor Cell Therapy in Peripheral Arterial Disease Current knowledge and controversies. Drs. M. Teraa , MD 1,2 Prof. dr. M.C. Verhaar , MD PhD 2 Prof. dr. F.L. Moll, MD PhD 1 1 Department of Vascular Surgery, University Medical Center Utrecht, The Netherlands

E N D
Stem and Progenitor Cell Therapy in Peripheral Arterial DiseaseCurrent knowledge and controversies Drs. M. Teraa, MD 1,2 Prof. dr. M.C. Verhaar, MD PhD 2 Prof. dr. F.L. Moll, MD PhD 1 1 Department of Vascular Surgery, University Medical Center Utrecht, The Netherlands 2 Department of Nephrology and Hypertension, University Medical Center Utrecht, The Netherlands
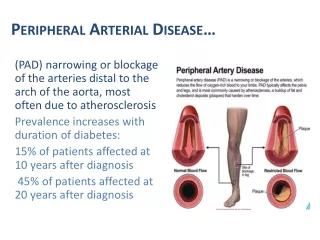
Backgrounds Critical Limb Ischemia (CLI) • Rest pain or tissue necrosis • 500-1000 individuals per million persons per year • Important functional implications • Major impact on quality of life: • Worse than in patients with terminal cancer, chronic kidney or heart disease • CLI is associated with significant morbidity and mortality: • 50% one year amputation free survival
Backgrounds CLI • ~40% of the patientsnoteligibleforsurgicalorendovascularrevascularization: • Anatomiclocation of the lesion • Extent of disease • Extensiveco-morbidity • No effectivepharmacologicaltherapy • Amputationoftenremainingoption New revascularizationstrategiesneeded Celltherapy is a promisingoption
Endothelial Progenitor Cells (EPC) EPCs and therapeuticimplications Pancreas Regeneration GlomerularCapillaryRepair Neovascularisation after ischemia Asahara, 1997 Rookmaaker, 2002 Gloerich, 2004
Gene and growth factor therapy • Pilot studies have shownpromisingresultsfor: • Vascular Endothelial Growth Factor (VEGF) • Hepatocyte Growth Factor (HGF) • Fibroblast Growth Factor (FGF) • Hypoxia Inducible Factor-1α (HIF-1α) • Larger trials have shownratherdisappointingresults Whataboutcelltherapy?
Celltherapy – TACT Study (2002) First Clinical trial • Pilot study (25 patients) • BM-MNC vs saline • Significantly improved ABI, TcPO2, rest pain, pain-free walking time at 4 and 24 weeks • Randomized trial (22 patients) • BM-MNC vs PB-MNC • Significant improvement for BM-MNC Adapted from Tateishi-Yuyama et al. Lancet. 2002;360(9331):427-35
Current results on cell therapy in CLI Mainlysmallnon-controlled studies Adapted from Fadini et al. Atherosclerosis. 2010;209(1):10-17
Needforconfirmation!!! • Largerandomizedcontrolled trials • More clinical relevant end points: • Amputation • Mortality • Quality of Life • Elucidate the black box of celltherapy
Black Box Patientcharacteristics? Administration route? Cell type? Cellsource? Mechanism?
Which patient will benefit? • Young vs. Old • Diabetics vs. Non-diabetics • Male vs. Female • Chronickidneydisease • BMI • Smokers vs. Non-smokers • Fontaine III vs. Fontaine IV • Buerger’sdisease vs. Atherosclerosisobliterans
The cell? • Clinicallystudied: • MobilizedPB-MNCs • BM-MNCs • CD34+ selectedcells • BM-MSCs (Bone marrow derived mesenchymal stem cells) Adapted from Fadini et al. Atherosclerosis. 2010;209(1):10-17
The way? • Intra-arterially or intra-muscular • Combined intra-arterial and intra-muscular • Once or repetitive administration • Amount of cells needed: • Feasibility versus effectiveness
Future perspectives for cell and source • Cellsources: • Blood • Bonemarrow • Fat • Cordblood • Embryonic • iPSCs (induced Pluripotent Stem Cells) • Cell types: • MNC • MSC • Cultured EPC: • Endothelial Colony Forming Cells (ECFCs) • Circulating Angiogenic Cells (CACs) Lu et al. DiabetesRes Clin Pract. 2011; [Epubahead of print]
Future perspectives in cell therapy • Progenitorcelldysfunction in cardiovasculardiseases • Pretreatment of cells could -partly- restore dysfunction: • Statins • Antioxidants • NO-donors • PPAR-γagonists Adapted from Sasaki et al. Proc NatlAcadSci USA. 2006; 103(39): 14537-41
Harvesting methods • Marrowminer: • Claims to harvest more progenitorcells • Commercial kits? Be aware: • GMP-guidelines • Aseptic isolation and culture • Knowledge of the product • Efficacystillnotestablished Clinical trials are still the way to go!!!
Large trials • 21 ongoing trials studying stem/bonemarrowcelltherapy in PAD • Significant commercial input Lawall et al. ThrombHaemost. 2010; 103(4): 696-709
JUVENTAS* Trial (NCT00371371) *ReJUVenatingENdothelial progenitor cells via Transcutaneous intra-Arterial Supplementation bone marrow (100 ml) bone marrow (100 ml) BM-MNC Infusion Placebo versus Storage
Juventas-trial Highlights • Started in September 2006 • Design with repeated intra-arterial infusion • Over 20 referring centers • Group sequential interim analyses for safety and efficacy • Coupled basic research Design • Randomized, placebo-controlled, double-blinded clinical trial Objectives • Evaluate the effects of repeated intra-arterial infusion of BM-MNC in 110 – 160 CLI patients • Study functional characteristics of BM-MNC and relate dysfunction to clinical outcome Currently 100 patients included!!!
JuventasStudy Group Steering Group Drs. M. Teraa Dr. R.W. Sprengers Prof. Dr. M.C. Verhaar Prof. Dr. F.L. Moll Dr. R.E.G. Schutgens Dr. I.C.M. Slaper-Cortenbach Prof. Dr. Y. van der Graaf Prof. Dr. W.P.Th.M. Mali Prof. Dr. P.A. Doevendans Dr. A. de Wit For more information: www.juventas-trial.nl Data Safety Monitoring Committee Prof. Dr. A. Algra Dr. I. van der Tweel Prof. Dr. T.J. Rabelink The JUVENTAS trial is made possible by grants of: Foundation ‘De DrieLichten’
Question 1 • Fromanembryonic point of view endothelialprogenitorcells are closestrelated to: • Neuralcells • Stromal cells • Haematopoieticcells • Adipocytes • Hepatocytes
Answer question 1 • From an embryonic point of view endothelial progenitor cells are closest related to haematopoietic cells (answer C). Both the primitive vasculature and haematopoietic cells develop from the blood ilands as a common origin. Endothelial progenitor cells do express both markers expressed on haematopoietic and endothelial cells further underlining their similar ontologic relation.
Question 2 • The most appropriateway to administerprogenitorcells in patientswithperipheralarterialdisease is: • Intramuscular • Intraarterially • Combination of A and B • Stillunclear
Answer question 2 • The most appropriate way to administer progenitor cells in patients with peripheral arterial disease is still unclear (answer D) Most studies conducted so far have studied the intramuscular method to apply cell based therapies. A smaller amount of studies performed intra-arterial infusion. Just one study analyzed a combination of both administration routes. Based on current evidence there seems no clear difference of the administration route applied. Intramuscular administration seemed to perform somewhat better, this was not significant however and needs to be confirmed in controlled studies. Fadini, Agostini, Avagaro. Atherosclerosis 2010; 209: 10-17
Question 3 • Basedoncurrentliteratureclinicaleffectsof celltherapy is notknown to beinfluencedby: • Cellsource • Number of cellsinfused • Underlyingcause of limbischemia • Sex
Answer question 3 • Based on current literature clinical effects of cell therapy is not known to be influenced by sex (answer D). Clinical effects (ABI, tcPO2) have been shown to be somewhat better in bone marrow derived cells and probably even better in bone marrow derived mesenchymal stem cells. Effects of cell based therapies have almost unequivocally been better with increasing amount of cells administered (mainly number of CD34+-cells). Moreover, ther underlying condition causing the critical limb ischemia clearly plays a role in the effects observed after cell therapy. Patients suffering from atherosclerosis obliterans have shown to be respond better than patients with thromboangitis obliterans. Sex has not yet been shown to influence effects observed after cell therapy. Lu, Chen, Liang et al. Diabetes Res Clin Pract 2011; Epub ahead of print Fadini, Agostini, Avagaro. Atherosclerosis 2010; 209: 10-17 Idei, Soga, Hata et al. Circ Cardiovasc Interv. 2011; 4: 15-25
Question 4 • What’strueaboutcellbasedtherapies in peripheralarterialdisease: • Celltherapy is widelyaccepted as a conventionaltherapy • Itseffectsonclinical relevant end pointsstillneed to beconfirmed • Malignanttransformation is a serious and commonreportedproblem in celltherapy • Growth factor therapiesseemequallyeffective
Answer question 4 • What’s true about cell based therapies in peripheral arterial disease: “Its effects on clinical relevant end points still need to be confirmed.” (answer B) Cell based therapies have generally shown to improve surrogate end points, such as ABI and tcPO2. Pain free walking distance, ulcer healing and amputation-free survival have also been reported to improve. Most studies conducted were small non-controlled studies and therefore not designed or underpowered to draw definitive conclusions on clinical relevant end points. Fadini, Agostini, Avagaro. Atherosclerosis 2010; 209: 10-17 Sprengers, Moll, Verhaar. Eur J Vasc Endovasc Surg 2010; 39: S38-43