Download
1 / 27
270 likes | 512 Views
Using Information Technology to Detect Ambulatory Adverse Events Related to Antidiabetic Drug Therapy. Judy Wu, PharmD Duke University Hospital. Co-Investigators: Heidi Cozart , RPh ; Julie Whitehurst, PharmD ; Philip Rodgers, PharmD ; Jennifer Mando , PharmD.

E N D
Using Information Technology to Detect Ambulatory Adverse Events Related to Antidiabetic Drug Therapy Judy Wu, PharmD Duke University Hospital Co-Investigators: Heidi Cozart, RPh; Julie Whitehurst, PharmD; Philip Rodgers, PharmD; Jennifer Mando, PharmD
Adverse Drug Events (ADEs) • Research primarily in the inpatient setting • 3 – 6 ADEs per 100 admissions1-3 • 27% – 50% of ADEs are preventable1-3 • Estimated cost: $ 3.5 billion (2006 dollars)4 • ADE detection methods • Chart review, patient surveys, computer event monitoring, text scanning, voluntary reporting • Multiple methods = more ADEs • Not well understood in other care settings Bates DW et al. JAMA 1995;274(1):29-34. Classen DC et al. JAMA. 1997;277(4):301-6. Jha AK et al. J Am Med Inform Assoc 1998;5(3):305-14. Aspden P, IOM (U.S.). Preventing medication errors. Washington, DC: National Academies Press, 2007.
the magnitude of the problem is likely to be greater outside the hospital.” “Most data on medication error incidence rates come from the inpatient setting, but - Institute of Medicine Aspden P, IOM (U.S.). Preventing medication errors. Washington, DC: National Academies Press, 2007.
Definitions Any error in any stage of the medication use process (ordering, transcribing, dispensing, administering, or monitoring) Bates DW et al. J Gen Intern Med 1995;10: 199-205. Adverse Drug Events (ADEs) Patient injury resulting from medical intervention related to a drug Bates DW et al. JAMA. 1995; 274:29–34. Medication Errors Gandhi TK et al. International Journal for Quality in Health Care. 2000; 12:69–76.
Scope of the Problem • Limited research in ambulatory care1,2 • Baseline ADE incidence rate • Identify strategies to decrease ADEs • Barriers to ambulatory care ADE research • Inefficient • Lack of accessible data • Large patient population • Most common medications resulting in ED visits • Insulin and warfarin3,4 Thomsen LA et al. Ann Pharmacother 2007;41(9):1411-26. Field T et al. Med Care 2005; 43: 1171-1176. Hafner J et al. Annals of Emergency Medicine. 2002; 30: 258-267. Budnitz DS et al. JAMA 2006;296(15):1858-66.
Research Objectives • Quantify hypoglycemia ambulatory ADEs resulting in emergency department visits or hospitalization • Characterize the population of subjects experiencing ADEs • Evaluate the utility of three different electronic adverse event detection methods • Design a catalog of trigger words to detect possible ADEs through free-text searching
Study Design • Retrospective, electronic chart review • Approved by Duke University Institutional Review Board • Study site: Duke University Hospital • Study period: January 1, 2007 to September 30, 2007 • Inclusion criteria • Subjects >18 years old experiencing possible antidiabetic drug-induced hypoglycemia resulting in an emergency department visit or hospitalization • Exclusion criteria • Subjects experiencing hypoglycemia not associated with medication use • Lack of objective evidence
Measurements • Hypoglycemic ADE • Blood glucose < 50 mg/dL while on antidiabetic therapy • ADE scoring • ADE = causality score ≥ 5 and a severity score ≥ 3 • Causality - Naranjo algorithm1 • Severity - Duke 7 point ADE severity score2 • ADE group • Comprehensive list of ADEs detected from any of the 3 tools Naranjo CA et al. Clin Pharmacol Ther. 1981;30:239-245. Kilbridge PM et al. J Am Med Inform Assoc 2006; 13: 372-377.
Detection Methods • Computerized ADE Surveillance (ADE-S) • Diagnosis (ICD-9) codes • Free-text searching
Detection Methods:Computerized ADE Surveillance • Logic based rules • Screens demographic and laboratory data, medications, and other clinical results • Alerts pharmacist about possible ADEs • Review and scoring process • Acute care setting vs emergency department • Hypoglycemia rule • Dextrose 50% when BG < 50 mg/dL
Detection Methods:Diagnosis (ICD-9) codes • Administrative data • International Classification of Diseases, 9th edition • Codes for diagnoses and procedures • E900 codes specific to adverse events due to drugs • E932.3 Adverse effect insulin/antidiabetics
Detection Methods:Free-text searching • Electronic medical records • Emergency department visits • Refinement of searching tool • Identification of trigger words • Elimination of negative and ambiguous terms • Final search strategy • Include {DMordiabetes} AND {hypoglycemiaor hypoglycemic or low blood glucose or low BG or low glucose} AND exclude {(-)DM}
Results: Hypoglycemia Alerts Detected n = 138 n = 212 12 112 168 6 8 26 32 # of unique alerts = 364 n = 72
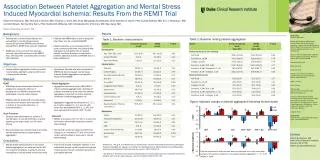
Results: Hypoglycemia ADEs Detected 91 55 Computer Surveillance 10 6 5 22 57 ADEs = 154 (42%)
ADE Distribution By Race n = 154
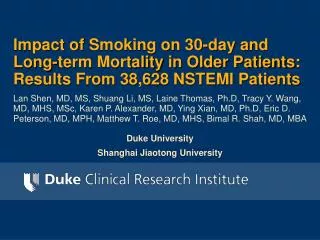
ADE Distribution By Age n = 154 Age (Years) Number of Events
ADEs With Insulin Involvement n = 154 Mean blood glucose value at time of hypoglycemic event: 32 mg/dL Insulin + Sulfonylurea 4.5%
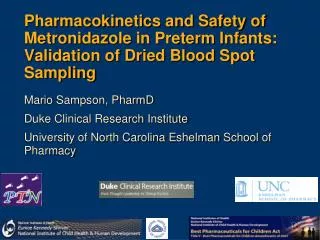
Positive Predictive Value (PPV) of ADE Detection Tools 55 ADEs 91 ADEs ‡ 40% 43% Computer Surveillance 100% 57 ADEs 79% ‡ Overestimation
Limitations • Retrospective, chart review • Not generalizable to other ambulatory ADEs • Subjectivity in scoring ADEs • Underestimation of hypoglycemic incidence rate • Specific population • Exclusion of symptomatic hypoglycemia with BG > 50 • Undetected hypoglycemic ADEs? • Detection tool limitations • ADE-S, ICD-9, free-text search
Conclusion • 17 hypoglycemia ADEs per month were detected • 49% require hospitalization • 71% of ADEs involved insulin use • African American and older age present more frequently with hypoglycemia ADEs • Highest yield & sensitivity free text search tool • Greatest PPV ICD-9 coding • Minimal overlap among tools • Combining methods increases ADE yield
“The primary focus of research on medication errors in the next decade should be prevention strategies, recognizing that to plan an error prevention study, it is essential to be able to measure the baseline rate of errors.” - Institute of Medicine Future research: • Expand into other populations and other ambulatory ADE areas • Tool refinement • Use of detection methods in outpatient clinics • Prevention strategies
Acknowledgements • Heidi Cozart • Julie Whitehurst • DHTS • Department of Pharmacy • Residency Research Committee
Race Distribution North Carolina Durham County Duke http://quickfacts.census.gov/qfd/states/37/37063.html
Race Distribution Actual Predicted http://quickfacts.census.gov/qfd/states/37/37063.html