Download
1 / 17
190 likes | 431 Views
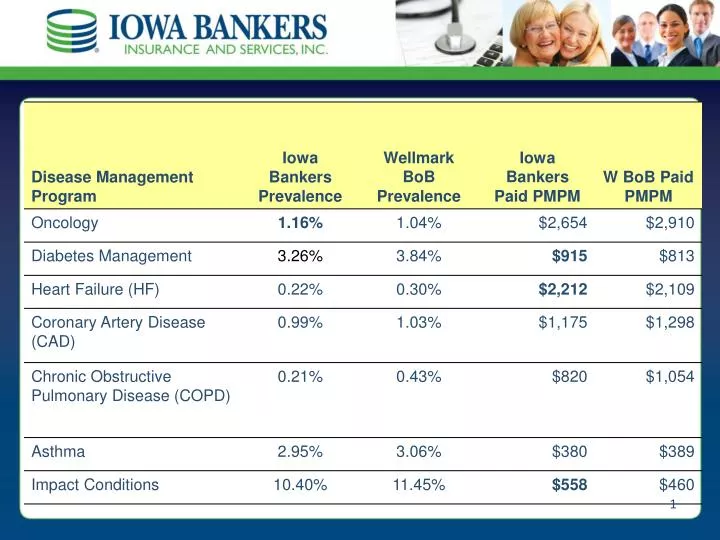
Comparing Iowa Bankers’ members diagnosed with conditions applicable to disease management programs (prevalence) and the amount of claims paid for those members per month, with the Wellmark book of business prevalence and costs:

E N D
Comparing Iowa Bankers’ members diagnosed with conditions applicable to disease management programs (prevalence) and the amount of claims paid for those members per month, with the Wellmark book of business prevalence and costs: The Iowa Bankers’ prevalence rate was greater than the Wellmark book of business for oncology conditionsonly. Claims paid per diseased member per month exceeded the Wellmark book of business for members with diabetes, heart failure, and impact conditions. Disease Management
Employee Benefit Workshop 2009 • National Trends • IBBP Information • Analysis of the Plan • Wellness
The Case for Disease Management • Chronic illness accounts for more than 75 percent of all health care costs.* • An estimated one in three Americans has some form of cardiovascular disease, which is responsible for direct and indirect costs of $431.8 billion dollars annually.** • Participants who better manage chronic diseases have a lower number of emergency room visits, hospitalizations and additional complications. * National Centers for Disease Control and Prevention ** American Heart Association, Heart Disease and Stroke Statistics, 2007
Managing a Chronic Disease is Complex • 95% of what a person with diabetes should do to maintain good health is self-directed • Only 1 in 5 are doing everything they should
Disease Management Programs • Diabetes • Congestive Heart Failure • Coronary Artery Disease • Asthma (high risk) • Chronic Obstructive Pulmonary Disease
Program Design Identification Stratification Assessment Intervention
Risk Stratification • 4 stratification levels • Level 1: Participants who are stable and at lowest risk for utilization, or aggravating their condition • Level 2: Participants who are at some risk for utilization, or aggravating their condition • Level 3: Participants who represent moderate risk for utilization or aggravating their condition, however, still preventable • Level 4: Participants at highest risk for utilization, or aggravating their condition, and timely action is required to lessen the risks
Welcome Process • Welcome kit • Personalized welcome letter • Health workbook • Quiet period • Welcome call • Care coordinators engage participants in the program after they are identified • Opt-out engagement model • Participant must choose not to participate
Address the “Whole Person” • It’s about people….not their disease • Depression • Co-morbidity • Working • Family • Denial • Trust channels are essential for outcomes improvement and successful behavior modification • Must establish unconditional credibility and positive intent to create change All co-morbidities and behaviors should be managed simultaneously by the same trusted relationship.
Personalized Interventions • Interventions, support, and stratifications are dynamic and based on current health status and behaviors of participant • Prochaska readiness to change • Set obtainable goals with member
Member Interventions * *Asthma member interventions vary slightly. **Disease specific newsletters are sent quarterly for all programs except Impact conditions.
Improving the Patient-Physician Relationship
Programs are Designed to Achieve Results Clear need for program Supported by evidence-based medicine Measurable outcomes
Member Satisfaction Above Benchmark 8.26Overall program satisfaction 85% Improvement in taking medications as prescribed 92%Have more information on their overall health