Download
1 / 34
340 likes | 523 Views
Building public health capacity within an integrated health care system. Ted Bruce Executive Director, Population Health. Outline of Comments. Brief history and components of public health renewal in Canada Main strategic initiatives Core services Knowledge transfer and information systems

E N D
Building public health capacity within an integrated health care system Ted Bruce Executive Director, Population Health
Outline of Comments • Brief history and components of public health renewal in Canada • Main strategic initiatives • Core services • Knowledge transfer and information systems • Human resource development
Key Messages • Developing public health workforce will be impeded if infrastructure is strained • Integration of public health within the health system remains an unrealized potential • Public health leadership must be more assertive in putting forth the evidence on the value of public health • Measuring and advocating on inequities is at the core of public health
Background • Growing concern that Canada’s Public Health infrastructure was neglected and deteriorating • Series of serious public health events: • Walkerton, Ont. - e.coli outbreak - May 2000 • N. Battleford, Sask.- Cryptosporidium outbreak -April ’01 • SARS – Spring 2003 • Series of national reports on public health system • The Naylor Report
CIHR Report (June2003) “The Future of Public Health in Canada: Developing a Public Health System for the 21st Century” • Examined structure of Canada’s public health system(s). • Advised how public health system could be better structured & resourced. • Identified 9 key infrastructure elements for effective, modern, comprehensive public health system.
Key Public Health SystemInfrastructure Elements • Clearly defined essential functions • Defined roles/responsibilities at each level (national, provincial/territorial, regional/local) • Consistent, modern legislation • Appropriate delivery structures • Appropriate funding levels • Appropriate numbers of well-trained staff • Information systems to support assessment and surveillance • Access to expertise and support • Accountability mechanisms at each level of the system
Contextual Factors Affecting Public Health In Canada • National and provincial jurisdictions • Integrated regional service delivery in most provinces • Primary care physicians not well integrated • Dominant medical model and strong interest groups • Strong national conceptual framework for public health • Creation of the Public Health Agency of Canada
Vancouver Coastal Health • 54,165 sq. kms • 1 million people • Richmond, Vancouver, North Shore, Sea to Sky, Sunshine Coast, Powell River and Central Coast • Provides full continuum of primary, acute and community care as well as many specialized tertiary and quaternary services
Safe, Healthy Communities and a Sustainable Environment For all British Columbians High Quality Patient Care Improved Health and Wellness for British ColumbiansA Sustainable,Affordable Health Care Systems Ministry of HealthGoals Government Strategic Goal Service Plan “Domains” Managing Disease & Disability Coping with End of Life Staying Healthy Getting Better Public Health Renewal Population Health Promotion Prevention in Primary Care SupportingSelf-Care BC’s Health System
Evidence Review Model Core Program Papers Performance Improvement Planning Reporting and Monitoring
Evidence Reviews Extensive Database Searches for intervention studies with a focus on cost effectiveness Include grey literature Application of evidence quality criteria Summarize evidence including best practice conclusions
Model Core Program • Contributing to the surveillance and monitoring of air quality, including trend analysis and assessment of public health reports. • • Identifying, with partners as appropriate, key air pollutants and sources (including new products), and assessing/prioritizing their public health impact. • • Identifying and implementing, with partners, effective interventions. • • Educational and awareness initiatives.
Performance Improvement Plan Enhance air quality data management Revise policies and procedures Mount air quality public education campaign Advance second hand smoke regulations
Core Competency Challenges • A high proportion of vacant public health positions • A significant proportion of practitioners working in public health who do not have specialized training in public health (e.g., many physicians working as medical officers of health do not have training in community medicine); • Inequitable distribution of public health resources within and between jurisdictions; • A distinct shortage of public health providers in First Nations communities; • Lack of surge capacity to respond to new and emerging health threats; and • Non-competitive remuneration
Core Competencies - Strategy • Improved health human resource reporting • Calls for a Canadian Plan – A new framework in 2004 • Development of core competencies
Public Health Sciences Assessment and Analysis Policy and Program Planning, Implementation and Evaluation Partnerships, Collaboration and Advocacy Diversity and Inclusiveness Communication Leadership Core Competencies
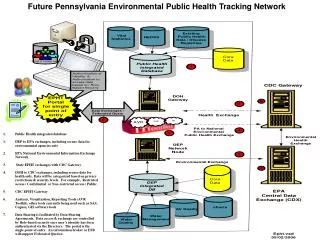
Knowledge and Information Capacity • Information Systems • Panorama • Communicable Disease and Immunization • 2008 • Real time ability to collect, share and analyze • Public Health Information Project BC • Expands to Family Health and to Environmental Health and Health Protection • Move eventually to Core Services
Information Systems - Challenges • Large infrastructure costs • Complexity of electronic medical record • Difficult to access administrative databases • Clarity on minimum data set difficult due to scope • Hard measures and soft measures
National Collaborating Centres • Knowledge Synthesis • Identification of Knowledge Gaps • Knowledge Translation • Network Development
National Collaborating Centres • Aboriginal Health sited at University of Northern British Columbia (UNBC), British Columbia; • Determinants of Health sited at St. Francis Xavier University, Atlantic; • Environmental Health sited at British Columbia Centre for Disease Control (BCCDC), British Columbia; • Infectious Diseases sited at International Centre for Infectious Diseases (ICID), Winnipeg; • Healthy Public Policy sited at Institut national de santé publique du Québec (INSPQ), Quebec; and • Methods and Tools sited at McMaster University, Ontario.
Knowledge Transfer Challenges • Complexity of Decision-Making • Lack of time • Culture of doing • Challenges in rural & remote areas • Tension over use of “real” money • System is undermanaged - AHFMR
Inequities in Health and Well-being in BC LE0 for BC Total Population (2001-2005) by Local Health Area (LHA) (Data source: BC Health Data Warehouse and BC STATS)
Health Inequities: Issues • Significant inequities in health status in BC - most notably Aboriginal people • Threat posed by growing gap in socioeconomic status between rich and poor Age/Gender-standardized Prevalence Rates per 100,000 Socioeconomic Inequities in Health: Diabetes in BC Cumulative Proportion of Population by Household Income Group (Data source: Statistics Canada Canadian Community Health Survey 2003)
Core Services – The Inequities Lens • Recognition of inequities and vulnerable populations • Increased emphasis on disease surveillance and health assessment – Linking health status and social determinants • Evidence Review • Advocacy Networks
The Lens • Does the initiative address the needs of a disadvantaged population? • Are populations affected differently by the intervention? • Are the effects of the initiative valued differently? • Is an effort made to minimize barriers? • Does evaluation of effectiveness include disadvantaged populations? • (Dans et al, 2005)
Health Impact Assessment • Renewed Interest Across Canada and OECD Countries • Quebec • BC Act Now Inter-Ministerial Committee • Opportunity To Contribute to Civil Society • “Making the right choice the easiest choice”
Issues Going Forward • Financing – 6% solution • Expectations of illness prevention and health and promotion • Leadership • Relationship with primary care
Key Messages • Developing public health workforce will be impeded if infrastructure is strained • Integration of public health within the health system remains an unrealized potential • Public health leadership must be more assertive in putting forth the evidence on the value of public health • Measuring and Advocating on Inequities is at the Core of Public Health