Download
1 / 15
150 likes | 287 Views
Master Class Lipid Innovations Prague, Czech Republic May 27-28 , 2011. The concept of Diabetes & CV risk: A lifetime risk challenge. The Clinical Significance of LDL-Cholesterol : No Longer a Hypothesis?. Presentation topic. Slide lecture prepared and held by:.

E N D
MasterClassLipidInnovations Prague, Czech Republic May 27-28, 2011 The concept of Diabetes & CV risk:A lifetime risk challenge The ClinicalSignificance of LDL-Cholesterol: No Longer a Hypothesis? Presentation topic Slide lecture prepared and held by: John J.P. Kastelein, MD PhD AcademicMedical Center Universityof Amsterdam Dept. VascularMedicine Amsterdam, The Netherlands
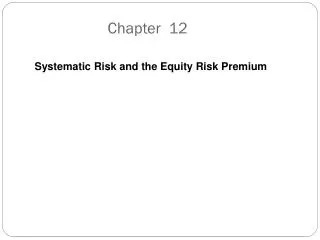
Mortality from Ischemic Heart Disease and Cholesterol 3,020 Deaths A. HDL-C B. non-HDL-C C. Total/HDL-C Age at risk(years) Age at risk(years) Age at risk(years) 128 70-89HR 0.69(0.63-0.74) 70-89 64 32 70-89 60-69HR 0.60(0.56-0.64) 60-69 16 8 60-69 40-69HR 0.56(0.51-0.60) 40-69 4 2 1 40-69 0.5 1.0 1.5 3.0 4.0 5.0 6.0 3.0 4.0 5.0 6.0 7.0 Usual HDL-C (mmol/L) Usual non-HDL-C (mmol/L) Usual total/HDL-C (mmol/L) Prospective Studies Collaboration. Lancet 2007;370:1829
Discovery of statins Discovery of LDL receptors Brown and Goldstein, 1974 Endo, 1976 Statins raise LDLreceptors in the liver Plasma LDL is reduced
Clear Cardiovascular Benefits of Intensive Lipid-Lowering Therapy POSCH-PL Primary prevention trials 4S-PL 25 Secondary prevention trials POSCH-Rx 20 CARE-PL 4S-Rx HPS 15 LIPID-PL Statin trials TNT-10A % Patients with CHD Event HPS-PL CARE-Rx WOSCOPS-PL 10 LIPID-Rx non statin trials TNT-80A WOSCOPS-Rx HPS-Rx LRC-PL 5 ASCOT-PL LRC-Rx ASCOT-Rx AFCAPS-PL AFCAPS-Rx 0 50 70 90 110 130 150 170 190 210 (mg/dL) 1.3 1.8 2.3 2.8 3.4 3.9 4.4 4.9 5.4 (mmol/L) LDL cholesterol
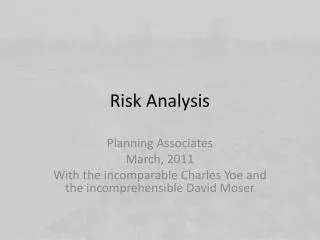
Correlation Between LDL-C Lowering and Decreased CHD Risk According to Treatment Modality in a Meta-Regression Analysis London Oslo MRC Los Angeles Upjohn LRC NHLBI POSCH 4Sa WOSCOPSa CAREa LIPIDa AF/TexCapsa HPSa ALERTa PROSPERa ASCOT-LLAa CARDSa 100 80 60 Nonfatal MI and CHD Death Relative Risk Reduction, % 40 20 0 –20 15 20 25 30 35 40 LDL-C Reduction, % CTTC: 23% reduction in major vascular events for 1mmol/L lower LDL-C with statins Adapted from Robinson JG, et al. J Am Coll Cardiol. 2005;46(10):1855–1862
Deaths Due to Suicide, Cancer, and Hemorrhagic Stroke *Number of patients: atorvastatin 10 mg/atorvastatin 80 mg †Fatal and non-fatal
Cardiovasculareventsoccurred in 22 (10%) of 227 patientswithabnormalliver tests whoreceived statin (3·2 events per 100 patient-years) and 63 (30%) of 210 patientswithabnormalliver tests whodidnotreceivestatin (10·0 events per 100 patient-years; 68% relative risk reduction, p<0·0001). Thiscardiovasculardisease benefit was greater (p=0·0074) thanit was in patientswithnormalliver tests Lancet, 2010; 376; 9756
GREACE: Enzyme Activity in Patients with Raised Liver Enzymes. A) On Statins B) Not On Statins Lancet, 2010; 376; 9756
Absolute Effect of Statin Therapy onMAJOR VASCULAR EVENTS Control 20 21% relative risk reduction per mmol/L Statin 15 15% relative risk reduction per 0.5 mmol/L More statin Five year risk of a major vascular event, % 10 Combined evidence: ~33% relative risk reduction per 1.5 mmol/L 5 0 0 1 2 3 4 5 LDL cholesterol, mmol/L
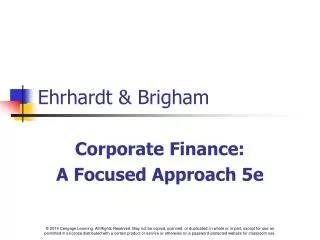
Proportional Effects on MAJOR VASCULAR EVENTS per mmol/L Reduction in LDL Cholesterol No. of events (% pa) Statin/ Contr ol/ Relative risk (CI) More statin Less statin 3485 (1.0) 4593 (1.3) 0.73 (0.69 - 0.78) Nonfatal MI 1887 (0.5) 2281 (0.6) 0.80 (0.74 - 0.87) CHD death Any major coronary event 5105 (1.4) 6512 (1.9) 0.76 (0.73 - 0.78) 1453 (0.4) 1857 (0.5) 0.75 (0.69 - 0.82) CABG 1767 (0.5) 2283 (0.7) 0.72 (0.65 - 0.80) PTCA Unspecified 2133 (0.6) 2667 (0.8) 0.76 (0.70 - 0.82) Any coronary revascularisation 5353 (1.5) 6807 (2.0) 0.75 (0.72 - 0.78) 1427 (0.4) 1751 (0.5) 0.79 (0.72 - 0.87) Ischaemic stroke Haemorrhagic stroke 257 (0.1) 220 (0.1) 1.12 (0.88 - 1.43) 618 (0.2) 709 (0.2) 0.88 (0.76 - 1.01) Unknown stroke Any stroke 2302 (0.6) 2680 (0.8) 0.84 (0.79 - 0.89) Any major vascular event 10973 (3.2) 13350 (4.0) 0.78 (0.76 - 0.80) 99% or 95% CI 0.4 0.6 0.8 1.2 1.4 1 Statin/more Control/less statin better statin better
0.94 (0.82 - 1.08) 0.88 (0.84 - 0.91) 0.90 (0.87 - 0.93) 0.90 (0.87 - 0.93) Relative risk (CI) Control/less statin better 1.5 1.25 1 0.75 Statin/more statin better 0.5 69 (1.7) 68 (1.6) 82 (0.4) 130 (3.4) 970 (2.4) 247 (1.2) 644 (8.0) 282 (1.1) 374 (1.8) 127 (2.4) Control/ 1825 (2.0) 6502 (2.4) 8327 (2.3) 4354 (2.2) 320 (17.9) 660 (14.0) Less statin No. of events (% pa) Statin/ 70 (1.6) 63 (0.3) 50 (1.2) 104 (2.7) 964 (2.4) 198 (1.0) 657 (8.2) 284 (1.2) 366 (1.8) 121 (2.3) 1768 (1.9) 5874 (2.2) 7642 (2.1) 3832 (1.9) 297 (16.8) 636 (13.5) More statin Difference between more vs less and statin vs control: 95% CI More vs less statin Statin vs control First cycle (14 trials) Subtotal (21 trials) Subtotal (5 trials) 0.4, p=0.53 99% or Total (26 trials) ALLIANCE PROVE-IT GISSI-HF AURORA SEARCH JUPITER ASPEN MEGA IDEAL A to Z = TNT 4D c 2 1 Proportional effects on ALL CAUSE MORTALITY per mmol/L LDL-C Reduction
Proportional Effects on CANCER INCIDENCE per mmol/L Reduction in LDL Cholesterol No. of patients Statin/ Control Relative risk (CI) Less statin More statin 0-1 year 982 (1.2%) 997 (1.2%) 0.98 (0.87 - 1.11) 1-2 years 1088 (1.3%) 1056 (1.3%) 1.03 (0.92 - 1.16) 2-3 years 982 (1.4%) 999 (1.4%) 0.98 (0.86 - 1.10) 3-4 years 873 (1.4%) 878 (1.4%) 0.97 (0.85 - 1.10) 4-5 years 680 (1.3%) 645 (1.3%) 1.05 (0.90 - 1.22) 5+ years 455 (1.5%) 489 (1.6%) 0.98 (0.80 - 1.21) All groups 5060 (6.0%) 5064 (6.0%) 1.00 (0.96 - 1.04) 2 0.01; p=0.94 c rend T = 1 0.5 0.75 1 1.25 1.5 Statin/more Control/less 95% CI 99% or statin better statin better