Download
1 / 27
280 likes | 1.72k Views
Advances in Supraglottic Airway. Dr. K. Sudarshan Consultant Anaesthetist Coimbatore. Which ones qualify ?. Should satisfy the following conditions. 1. Placed above the vocal cord level 2. Those devices which allow hands-free maintenance of an open airway

E N D
Advances in SupraglotticAirway Dr. K. Sudarshan Consultant Anaesthetist Coimbatore
Which ones qualify ? Should satisfy the following conditions
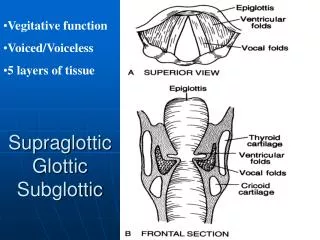
1. Placed above the vocal cord level 2. Those devices which allow hands-free maintenance of an open airway 3. Allows spontaneous or assisted ventilation
1908 to date • 1908- Hewitt Airway • 1913- Connell • 1915- Lumbard • 1916 – Mona Roberts • 1923 - Phillips • 1924 – Poe • 1930 – Waters insufflation • 1933 – Guedel • 1957- Fink vallecular • 1957 – Safar Airway • 1977 – Berman intubating • 1982 – Patil Syracuse • 1983 – Laryngeal Mask – Archie brain • 1985 – Combitube
Sir Frederic William Hewitt 1856 - 1916 A modified version of the original Hewitt airway The original Hewitt airway as it appeared in the February 15, 1908 issue of The Lancet.
COPA COMBITUBE NASOPHARYNGEAL AIRWAY
Advancements • New generation LMA’s • I gel • Laryngeal Tube/ King LTS/ LTD • Cobra plus tube
Generally demonstrate • Ability to be placed without direct visualization • Better cardio vascular stability both during insertion and removal • Minimal IOP and ICP changes • Provide little protection against aspiration • Contraindicated in full stomach patients
Has two separate tubes Three dimensional inflation of cuff Holds a better cuff seal pressure Proseal & LMA Supreme
Flexometallic tube Preformed angle Better placement Less incidence of dislodgement once placed More useful in head and neck surgery Flexible & Ambu LMA
Allows intubation with minimal head and neck manipulation Recommended in both difficult airway and Resuscitation algorithm C Trach allows intubation under direct vision ILMA & LMA C Trach
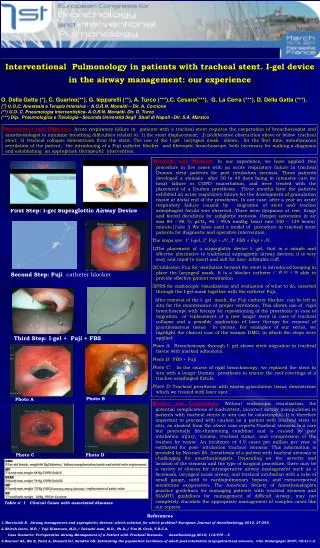
Single use, cuffless Integral gastric channel Epiglottic blocking ridge Moulding feature
Insertion Technique I GEL INSERTION http://www.youtube.com/watch?v=8jqHCnThf1E I GEL insertion in Lateral position http://www.youtube.com/watch?v=uLtSojaSX6c
Use lateral approach Introduce the tip into corner of mouth Advance behind the base of tongue Without exercising excessive force, advance until the base of the connector is aligned with teeth. Inflate the cuff INSERTION STEPS
Laryngeal tube Insetion. • http://www.youtube.com/watch?v=cBpU_fJe6ZA
Distal end has softened openings Used for both spontaneous and controlled ventilation Serves as a rescue airway Cobra plus tube
Cuffless Lines the pharynx Large internal volume –Allows collection of secretion, minimize aspiration Streamlined liner of Pharyngeal airway - SILPA
Summary • Provides hands free maintenance of airway • Can be used for both spontaneous and controlled ventilation • Provide little protection against aspiration • Useful in • Routine anaesthesia • emergency airway management • Aid to intubation
THANK YOU doctorsudarshan@gmail.com