Download
1 / 51
510 likes | 703 Views
SIGNS AND SYMPTOMS OF GIT DISORDERS. M. JUFRI MAKMUR. DEFINITION. Symptom : Subjective data of patient’s complaints Symptom is the most important thing in directing or guiding a diagnostic (60%) Sign : Objective data of physical findings

E N D
SIGNS AND SYMPTOMS OF GIT DISORDERS M. JUFRI MAKMUR
DEFINITION Symptom : Subjective data of patient’s complaints Symptom is the most important thing in directing or guiding a diagnostic (60%) Sign : Objective data of physical findings Refferences: Adam’s Physical Dx HarissonSigns &Symptoms Barbara Bates A Guide to Physical Examination and History Taking
Diagnostic Procedure SOAP S Subjective (identity, symptoms, clinical history, genetics) O Objective (signs, laboratory, radiologic, etc) A Assesment (diagnostic & DD) P Planning (treatment, supporting examination)
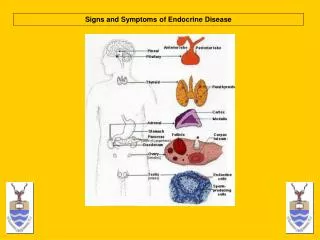
Basic of Symptoms and Signs Anatomical - topography - vascularization Physiological - organ function - metabolism
TOPOGRAPHYAbdominal regionsnine regions system RHC LHC EPI RL LL UMB RI LI SP
Organ Function Esophagus - swallowing Gaster & Duodenum - digestive and absorbtion Liver - anabolism and catabolism - detoxification - eritropoesis extramedullar - bile secretion
Pancreas - hormone secretion - enzyme secretion • Colon - reabsorbtion - faecal formation • Rectal - faecal reservoar
SYMTOMPS • 1. Abdominal pain • 2. Abdominal distension • 3. Dysphagia • 4. Odinophagia • 5. Hiccup or Singultus • 6. Vomitus & Regurgitasion • 7. Bloating • 8. Hematemesis • 9. Melena • 10. Diarhea • 11. Constipation • 12. Hematochezia
1. Abdominal pain - the most common symptom - location, type, cont. or intermitten, spread, referred - location depend on topographyc - due to : GIT ,TUG, Gyn, MSC, & CV - intermittent pain related to luminar organ (colic) - referred pain depend on innervasion
Types of abdominal pain: - epigastric pain gastroduodenitis, pancreatitis, Inferior MCI, left liver abcess, hepatic disorders, lymphoma, aneurisma aorta - Biliary colic pain from the right hypochondrial spread to right back shoulder gallstone & CBD stone
- Renal colic pain from back CVA spread to right iliac region obstructive uropathy - Right hypochondrial pain hepatic disorders, gall disorders, pleuritis, TUG disorders, and colon disorders
- Left hypochondrial Pain gastritis, pseudocyst pancreas, colon disorders TUG disorders, pleuritis, and spleen disorders - Umbilical pain gastritis, enteritis, colitis, aneurisma aorta, trombosis of mesenteric artery - Right & Left Lumbal pain colon disorders , TUG disorders, psoas abcess
- Right Iliac pain appendicitis, colon disorders, psoas abcess, PID, ovary cyst, ileitis term., TUG dis. - Left Iliac pain colon disorders, psoas abcess, PID, ovary cyst, TUG disorders
- Suprapubic pain cystitis & bladder stone, gynaecologic disorders, prostat disorders, colo-rectal disorders - Whole abdomen pain peritonitis, muscle pain, gastroenteritis, colitis
2. Abdominal Distention Due to: gas, fluid, mass, organomegali With or without pain ? Acute, recurent, or chronic ? Bowel or micturia alteration ? Organ involved: GIT, TUG, Heart
3. Dysphagia Difficulty swallowing Due to pain, obstruction, abn. peristalsis, or impaired reflex (nerve) Organ involved esophagus or oropharynx Most common case: Stricture esophagus, malignancy, GERD, multiple sclerosis
4. Odinophagia Pain of swallowing Organ involved esophagus Due to inflammation process
5. Hiccup or Singultus • Involuntary spasmodic contraction of the diaphragm followed by sudden closure of glottis • Due to increase of intracranial pressure, abdominal distention, gastric dilatation or inflammation, and renal failure, decrease serum levels of carbondioxide
6. Vomitus & Regurgitation Reflux of gastric contents The difference with or without contraction Involved vagal mechanism Non specific all of GIT disorders
7. Bloating • Full sensation of stomach • Due to inflammation, gastric emptying disorders, gastric mass, Increase of gastric pressure, increase of gas production, full or partial obstruction
8. Hematemesis Bleeding of upper GIT (lig. treitz) Due to variceal rupture, ulcer, erotion, mass Organ involved esophagus, stomach, & duodenum Life threatening symptoms
9. Melena • Black bloody stool from upper GIT • Black color is due to oxidation of Hb • Caused and organ involved similar to hematemesis • Life threatening symptom
10. Diarrhea Waterry stool more than 3 x/day Acute or chronic ? ( 2 weeks ) Due to reabsorbtion impairment (osmotic, toxin,etc) or hyperperistaltic (hyperthyroid) Organ involved Intestinal and colorectal
11. Constipation No defecation more than 3 days Due to obstruction, hypoperistaltic, inflammation, medication Organ involved Colorectal
12. Hematoschezia Fresh red bloody stool Due to lower GIT Haemorhoid is the most common cause of hematoschezia Acute,reccurent, or chronic ? Bowel habit alteration ?
Signs From physical findings Most common in hepatobilliary disorders General : vital sign Specific : inspection, palpation, percusion, and auscultation Gentle Right side of patients
1. Mental Change Most common in end stage of cirrhosis or severe hepatic disorders Called as encephalopathy hepatic Due to false neurotransmitter (aromatic amino acids, ammonia) Sometimes accompanied by flapping tremor
2. Icteric or Jaundice A yellow discoloration of the skin, mucous membranes, or sclera of the eyes Signs of excessive levels of conjugated or unconjugated bilirubin in the blood Type : Prehepatic, Hepatic, and Posthepatic Commonly accompanied by pruritus because bile pigment damage sensory nerve (hepatic or posthepatic jaundice)
Tea dark colored urine, clay colored stools always accoppany obstructive or posthepatic jaundice Prehepatic jaundice hemolysis Hepatic jaundice hepatic disorders, congestive liver (heart), systemic inflammation (sepsis, lupus), malignancy, and drugs Posthepatic jaundice CBD stone, malignancy of billiary system, lymphoma
3. Gynecomastia Occuring only in males Increased breast size due to excessive mammary gland development Most common in cirrhosis Failure to inactivate circulating estrogen
4. Spider Nevi/Angioma • A fiery red vascular lession with an elevated central body and a surrounding flush • Most common in face, neck, and chest • Related with cirrhosis and hyperestrogenemia (pregnancy)
5. Palmar Erythema Local vasodilatation along palmar side Most common in cirrhosis Mechanism is unknown
6. Ascites Accumulation of fluid in abdominal cavity Due to decrease of osmotic pressure (hypoalbumin) or increase of hydro-static pressure (portal hypertension) Signs dullness in both flank, shifting dullness, undulation Nonspecific sign Most common in cirrhosis, gynaecologic dis., severe diseases, peritoneal tuberculous, renal and heart problem
Ascites ascites accumulation of fluid in the abdominal cavity
7. Meteorismus Accumulation of gas in abdominal cavity Hypersonor percusion Bowel sound ? Metalic sound ? Pain ? Flatus ? Bowel Habit ? Due to electrolyte imbalance, drug, inflammation, total or partial obstructive
8. Pain palpation Depend on tophographic Types: Murphy’s sign, Ludwig’s sign, CVA percussion pain, epigastric pain, Mc Burtney’s pain, defanse muscular, suprapubic pain
9. Hepatomegaly • Hepatic enlargement subcostal • Confirmed by palpation, percussion, and sonographic • Due to systemic or hepatic problems • Important things size, consistency, and pain
LIVER SPAN MCL PERCUSSION NL < 12-13 CM 2-3 CM DURING INSPIRATION AND EXPIRATION COPD PALPATION PERCUSSION SCRATCH TEST LIVER SPAN MAY VARY BETWEEN OBSERVERS DEPENDING UPON WHERE THE MCL IS DETERMINED JAMA 1994;271:1859-1865
PALPATION FLEX KNEES AND HIPS IF POSSIBLE BEGIN LOW ON ABDOMINAL WALL AND MOVE HAND CEPHALAD, HAVE PATIENT TAKE A DEEP BREATH NOTE CONSISTENCY (NODULES, SMOOTH) AND CONTOUR IF THE LIVER EDGE IS FELT NOTE IF THERE IS ANY PAIN WITH PALPATION AUSCULTATE MOSBY’S GUIDE TO THE PHYSICAL EXAMINATION, 3RD ED. 1995
10. Splenomegaly Enlargement of spleen below of arcus costae Due to infection, trauma, portal hypertension, neoplastic, hematologic disorders Confirmed by palpation and sonograph
11. Mass palpation • Depend on topographic (similar to abdominal pain) • Important things size, consistency, mobility, and pain • Confirmed by sonograph, radiograph, and endoscopy
12. Flapping Tremor Patognomonis sign of encephalopathy hepatic Tremor of wrist joint after full extension
13. Pitting Edema • Accumulation of fluid in subcutis especially in plantar pedis • Due to hepatic, renal, heart, malnutrition, blood vessel, and systemic inflammation
Case Simulation • This lady have a fever since 1 weeks ago, abdominal distention in epigastric, vomitus, history of bloody diarhea, no history of dyspepsia before • What examinations should you perform to this patients? A young lady, married, 32 yo, came to hospital with chief complaint of epigastric pain localized What questions should you ask to this patient?
From examination, there are icteric, pain and palpable mass in epigastric, dark tea color urine, no cley-color stool, no defanse muscular What working diagnostic and differential diagnostic are possible in this patient?
The working dignostic in this patient is left lobe hepatic abcess • The differential diagnostic are pancreatic neoplasm, gastric mass, pseudocyst of pancreas, left lobe hepatoma, colon mass, lymphoma, aortic aneurism. • What are next examinations you suggested to confirm a diagnostic ? • What is the treatment ?