Download
1 / 61
610 likes | 1.02k Views
Streamlining ABO Antibody Titers For Monitoring ABO Incompatible Kidney Transplants. Wei Cai, M.T. (ASCP) wcai2@jhmi.edu Johns Hopkins Medical Institution. 监测 ABO 不相容性肾移植的 ABO 血型抗体滴度 约翰 霍伯金斯医学院 蔡伟. Background Information. Johns Hopkins Hospital Department of Pathology

E N D
Streamlining ABO Antibody Titers For Monitoring ABO Incompatible Kidney Transplants Wei Cai, M.T. (ASCP) wcai2@jhmi.edu Johns Hopkins Medical Institution
监测ABO不相容性肾移植的ABO血型抗体滴度约翰 霍伯金斯医学院蔡伟
Background Information • Johns Hopkins Hospital • Department of Pathology Transfusion Medicine Division • Specialist in Blood Bank Technology AABB (American Association of Blood Banks) • ABO Incompatible Kidney Transplant Program
背 景 知 识 约翰 霍伯金斯大学医院 病理系 输血医学部 美国血库协会 血库技术专家 ABO 血型不相容性肾移植计划
Crossing the ABO Barrier for Kidney Transplants As of May 25, 2007: 75,711 patients awaiting kidney transplantation In 2006, 17,092 kidney transplants were performed (6,433 or 37.6% living donors): Group O 7,662 A 6,354 B 2,255 AB 821
克服ABO血型障碍进行的肾移植 至2007年5月25日止, 有75,711名病人在等待进行肾移植2006年 进行了17,902个肾移植,其中6,433约37.6%是活体肾移植血型 肾移植 O 7,662 A 6,354 B 2,255 AB 821
In 2006, 4,056 patients died waiting for a kidney transplant, or 11.1 patients died per day 2,049 Group O 1,250 Group A 629 Group B 128 Group AB Deaths on Waiting List
在等待中死去的病人 2006年,共有4,056名等待肾移植的病人死亡,即每天有11.1名病人在等待中死去。
等待尸肾移植的病人数及等待时间 至07年5月25日 登记 等待 5年或5年以上 所有血型 75,711 8,079 O 39,713 4,459 A 21,457 1,844 B 12,379 1,592 AB 2,162 184
Cadaveric Kidney Transplant Wait • If registered in 2001-2002, median wait times as of May 25, 2007
2001-2002年间登记的病人, 到2007年5月25日平均等待时间是
Objectives • Expand donor pool and availability of organs for transplantation • Decrease time on organ waiting list • Circumvent hyperacute rejection and/or AMR (due to ABO and/or HLA antibodies) by developing immunomodulatory protocols • ABO incompatible • Donor-recipient with positive crossmatches (HLA) • Posttransplant patients who develop AMR (HLA)
目 的 • 扩大器官捐献群体及移植器官的来源 • 减少器官移植的等待时间 • 通过免疫调节方案,防止超急性排斥反应及/或因ABO血型或HLA抗体介导的排斥反应 • ABO不相容性 • 供-受者交配反应阳性(HLA) • 病人移植后出现抗体介导的排斥反应(HLA)
ABO Incompatible Transplantation • Based on Japanese experience • Based on our experience/protocol for crossmatch positive donor/recipient pairs and antibody-mediated rejection • Facilitated by laparoscopic donor nephrectomy • Preparative regimen with intensive follow up pre/postoperative plasmapheresis IVIgG and immunosuppression
ABO不相容的移植 基于日本的经验 基于我们对交配阳性的供-受者和抗体介导的 排斥反应的经验/方案 腹腔镜捐献者取肾促进了该类移植 强化随访的予处理方案 术前/后血浆置换 静脉注射IgG和免疫抑制
Reference ABO不相容性肾移植的长期结果
ABO不相容性病人在亲属活体肾移植后抗-A、B的滴度变化ABO不相容性病人在亲属活体肾移植后抗-A、B的滴度变化
Our Program- InkTp • Specialized Incompatible Kidney Transplant service and clinic • Weekly interdisciplinary rounds, composed of blood bank, apheresis service, HLA lab, nephrology, transplant surgery, pharmacist, psychologist, and social worker
我们的不相容肾移植项目 专业化的服务和临床 每周跨科的综合查房,包括血库、单采、HLA实验室、肾科、移植外科、药剂师、心理学家和社会工作者
Our Protocol • Modified from the Japanese protocol • Initial evaluation • donor and recipient medical, psychological and social work evaluations • HLA and ABO typing and titers • Review at weekly meeting • determination of optimal donor (HLA vs ABO) • treatment plan established
我们的方案 根据日本方案改进 初步评价 捐献者和受者进行医学、心理和社会服务的 评估 HLA和ABO分型及抗体滴度分析 每周会议的评述 根据HLA与 ABO相配情况决定最佳捐献者 建立治疗方案
Treatment Plan • Immunosuppression, may include splenectomy • All patients vaccinated (pneumococcus, meningococcus, haemophilus influenzae), regardless of splenectomy status • Pheresis plan established (number of procedures pre and postop)
治 疗 方 案 免疫抑制,可能包括脾切除 不管是否脾切除,所有病人接种疫苗(肺炎球菌、脑膜炎球菌、流感嗜血杆菌 ) 建立置换计划(术前/术后的置换程序和次数)
Plasmapheresis • Removes natural anti-A and/or anti-B antibodis • Both preop and postop procedures • Remove 1 plasma volume • Replace at 100% of volume removed • Replace with 5% albumin • except procedures immediately pre- and post- surgery, replace with plasma
血 浆 置 换 • 去除天然的抗-A/抗-B抗体 • 术前/后都进行置换 • 去除一个血浆容量 • 等量替换 • 用5% 的白蛋白置换 • 除术前/后立即的置换外,只用血浆置换
ABO Antibody Titer Goals • Pretransplant goal: titer 16 or less • Posttransplant • Continue to monitor ABO antibody titers • Significance in prediction of antibody mediated rejection is uncertain
ABO抗体滴度目标 • 移植前目标: • 滴度≤16 • 移植后 • 继续监测ABO抗体滴度 • 对于预测抗体介导的排斥反应的意义仍不确定
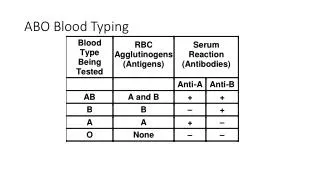
ABO Antibody Titers Conventional test tube method • AABB technical manual15th ed. Bethesda: American Association of Blood Banks, 2005. • Serial dilutions of each sample were prepared in 0.9% saline • Pooled indicator cells (Immucor, Norcross, GA) of the appropriate ABO type were added • 30 minutes 22C incubation test phase • 30 minutes 37C incubation test phase • AHG test phase using monospecific anti-IgG (Immucor, Norcross, GA) • Agglutination was scored using the Marsh 0 to 12 scoring system • AHG titer endpoint was the reciprocal of the highest dilution demonstrating macropscopic (score 3) agglutination
ABO抗体滴定 常规的试管法 • AABB技术手册 • 样品用0.9%的盐水进行连续稀释 • 加入适量的混合ABO血型指示细胞( Immucor ,Norcross, GA ) • 22度孵育30分钟 • 37度孵育30分钟 • 单特异性抗-IgG (Immucor, Norcross, GA) 的抗人球蛋白(AHG)实验阶段 • 用Marsh 0到12打分系统给凝集打分 • AHG最终滴度是样品出现肉眼可见的(3分)凝集的最高稀释倍数
ABO Antibody Titers • It is time consuming • Turn around time is critical • Our experience indicates that only the AHG titer values are critical • Titer endpoint is demonstrated with a macroscopic agglutination
ABO抗体滴度 • 这是一个花费时间的实验 • 关键是出现结果的时间 • 我们的经验表明只有AHG滴度是关键值 • 最终滴度是由肉眼可见的凝集决定
Objectives • The goal of the present study was to streamline ABO antibody titer determinations by assessing AHG titers using 1) A revised test tube method where the room temperature incubation phase was eliminated 2) An anti-IgG gel microcolumn method
目 的 • 本研究的目的是通过评估AHG 滴度,系列测定ABO抗体 1) 应用不需要室温孵育过程的改良试管法 2) 应用抗-IgG凝胶微柱法
Material and methods Revised test tube titration method • Serial dilutions of each sample were prepared in 0.9% saline • Pooled indicator cells (Immucor, Norcross, GA) of the appropriate ABO type were added • 30 minutes room temperature was omitted • Titers were incubated for 30 minutes 37C and then converted to the AHG test phase using monospecific anti-IgG (Immucor, Norcross, GA) • Agglutination was scored using the Marsh 0 to 12 scoring system • AHG titer endpoint was the reciprocal of the highest dilution demonstrating macropscopic (score 3) agglutination
实验材料和方法 改良的试管法 • 每个样品用0.9%的盐水进行系列稀释 • 加入适当的ABO血型的混合指示细胞( Immucor ,Norcross, GA ) • 省略室温30分钟孵育 • 37度孵育30分钟后用单特异性抗-IgG 进行AHG实验 • 用Marsh打分系统对凝集进行打分 • AHG最终滴度是样品出现肉眼可见的(3分)凝集的最高稀释度的倒数
Material and methods Anti-IgG microcolumn gel method • Serial dilutions of each sample were prepared • Twenty-five microliters of each plasma dilution and 50 microliters of 0.8% indicator red cells prepared in MTS™ Diluent 2 were added to the gel card microcolumns • After incubation at 37C for 15 minutes, the gel cards were centrifuged for 10 minutes • The titer endpoint was the reciprocal of the highest dilution demonstrating 1+
实验材料和方法 抗-IgG微柱凝胶法 • 每个样品系列稀释 • 在微柱凝胶卡中加入25微升每一稀释度的血浆和50微升应用MTS™稀释液2制备的0.8%的指示红细胞。 • 37℃孵育15分钟后将凝胶卡离心10分钟 • 最终滴度是显示1+凝集的最高稀释度的倒数
Anti-IgG Microcolumn Gel Cards Micro Typing Systems, MTS™, Ortho Clinical Diagnostics, Raritan, NJ, USA
抗-IgG微柱凝胶卡片 Micro Typing Systems, MTS™, Ortho Clinical Diagnostics, Raritan, NJ, USA 微型血型仪
Patient samples • Serial EDTA plasma samples from patients in our ABO INKT program • Fifty samples with anti-A and/or Anti-B antibodies • AHG titers ranging from 2 to 512 • 18 of the 50 (36%) samples were selected with titers of 16
病人样品 • 我们 ABO不相容的肾移植项目的病人EDTA血浆标本 • 50个有抗-A/抗-B抗体的标本 • AHG 滴度在2-512之间 • 50个中有18个样本滴度为16