Download
1 / 50
500 likes | 517 Views
"Equip practice nurses with knowledge and skills to assess, test, and manage vaginal discharge, STIs, and sexual health issues. Boost awareness of STI testing and sexual health services, emphasizing patient confidentiality and consent."

E N D
Aim For you to have the knowledge to assess, test and manage vaginal discharge and simple STIs in your patients
You will • Be aware of opportunities for STI testing • Consider why you should, and how you will incorporate sexual history taking into your consultations • Have some knowledge of Sexual/vaginal infections and how to screen/test for common infections • Understand the implications of manging your results correctly • Be aware of local sexual health service provision
Sexual Health Sexual health is a state of physical, mental and social well-being in relation to sexuality. It requires a positive and respectful approach to sexuality and sexual relationships, as well as the possibility of having pleasurable and safe sexual experiences, free of coercion, discrimination and violence
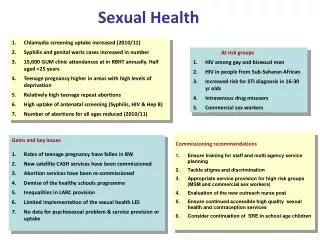
Sexual health is a UK government priority HIV continues to be one of the most important communicable diseases in the UK. The number of people living with HIV in the UK continues to rise and Around 1 in 4 of those infected are unaware of their infection. General practice has a role in caring for patients with HIV and assessing the risk of having undiagnosed HIV The scale and impact of the under-diagnosis of Hepatitis B and C is apparent
STI testing has moved towards self-taken swabs and home sampling • Rates of sexually transmitted infections (STIs) continue to rise, in some cases dramatically • There are serious implications for health
General practice is the largest provider of sexual and reproductive health care (SRH) in the UK RCGP 2017
General Practice is uniquely accessible. You need to discern people at high risk of having a sexual health problem from those with zero risk • GPs and practice nurses may be unaware of the extent of their lack of knowledge in what is a very rapidly changing field • Many lack confidence in discussing sexual health with their patients and lack time-efficient strategies
Screening/Testing for Sexual Infections in your setting When?
Referred by GP Vaccinations Screening for STIs New patient registration Post natal checks Any consultation! Cervical screening Repeat contraception Health education and prevention advice Chronic disease/medication reviews
Young/Vulnerable people Confidentiality Consent Fraser competent Capacity to consent to SI Adult/child safeguarding CSE Domestic violence Honour based violence Trafficking The law
Consent Children under the age of 16 can consent to medical treatment if they have sufficient maturity and judgement to enable them fully to understand what is proposed. This was clarified in England and Wales by the House of Lords in the case of Gillick vs West Norfolk and Wisbech AHA & DHSS in 1985
Fraser Guidance • the young person will understand the professional's advice • the young person cannot be persuaded to inform their parents • the young person is likely to begin, or to continue having, sexual intercourse with or without contraceptive treatment • unless the young person receives contraceptive treatment, their physical or mental health, or both, are likely to suffer • the young person's best interests require them to receive contraceptive advice or treatment with or without parental consent
Take a sexual history from a maleor female patient in a way • that is • Private and confidential • Non-judgemental • Responsive to the reactions of the patient • Avoid assumptions about • Sexual orientation • Gender/age of the partner(s) • Disability • Ethnic origin
The initial greeting to the patient • Maintain eye contact (if culturally acceptable) • Use appropriate body language • Initiate consultation with open questions followed by exploration of initial concerns and more closed questions as the consultation continue • Explain the rationale for some of the questions asked • Sexually explicit language • Use language that is clear and understandable • Both clinician and patient are comfortable • Possibility of anxiety and distress from the patient • Recognise non-verbal cues
Sanjit who is 44 is referred by the GP for triple swabsShe has had a horrible smelling discharge for the past 2 monthsShe is feeling very itchy and sore.She believes that this is due to her IUDShe has been treated with a canestan pessary twiceIt helped for a short while, but comes back
What should you ask? • Medical history • Medicines • Allergies • Menstrual history • Contraception • LMP • Other symptoms
Other symptoms? • Consistency of discharge • Nature of odour • Urinary problems • Pain • Bleeding • Lumps,rashes,ulcers
Blood Born Virus risks • Number of Partners last 3/6/12 months • Hepatitis B vaccianation • Previous HIV test • MSM or contact with MSM • IVDU or contact with IVDU • Snorting drug use • Chemsex
SI with people from high risk countries • Paid for sex • Been paid for sex • Sex with HIV+ person • History of coercive or non-consensual SI • Non-professional tattoos or piercings • Blood transfusion / medical procedures abroad
Recognise sexual health emergencies • CSE • Emergency contraception • Post-exposure prophylaxis (PEP) in HIV prevention, • Hepatitis B vaccinations • Responding to early presentation of rape and sexual assault
Window periods Chlamydia/Gonorrhoea: 2 weeks HIV: 4 weeks Syphilis: 12 weeks Hepatitis B/C: 3-6 months
Change in Vaginal Discharge • Candida or thrush • Bacterial vaginosis (BV) • Trichomonas vaginalis (TV) • Herpes • Gonorrhoea • Chlamydia • Physiological • Retained condom, tampon or foreign body
Signs & Symptoms • Offensive “fishy” smelling vaginal discharge. • More noticeable following sex. • Not associated with soreness or irritation.
Bacterial Vaginosis • Commonest cause of abnormal discharge in women of child bearing age. • Caused by an imbalance in vaginal ecology. • Risk factors include: • Vaginal douching • Using highly perfumed washing products • Recent change of sexual partner • Smoking
Treatment • Metronidazole 400mg orally bd for 5 days. • Intravaginal Metronidazole gel - once daily for 5 days. • Intravaginal Clindamycin 2% cream – once daily for 7 days. • Balance Activ gel (various regimes) • Avoidance of highly perfumed washing products.
Vulvovaginal Candidiasis • Thrush
Signs & Symptoms • Vulvitis • Vulval itching • Superficial dyspareunia • Dysuria • “Curdy” white, non offensive vaginal discharge. • Fissuring
Treatment • Clotrimazole 500mg pv stat pessary. • Clotrimazole 1% cream, topically. • Daktacort cream, topically (if severe erythema). • Oral fluconazole or itraconazole. • Avoidance of highly perfumed washing products.
Signs & Symptoms • Dysuria • Vaginal or urethral discharge • Abdominal pain • PCB/IMB • Up to 80 % Asymptomatic
Chlamydia Trachomatis • Epidemiology • 3-5% of all women attending GP surgery • 10% Under 25s • Risk Factors • Under 25 • New partner • > 1 partner in previous year • Contraception • TOP
Complications • Pelvic Inflammatory Disease (PID) • Adult or neonatal conjunctivitis • Sexually Acquired Reactive Arthritis (SARA) • Epididimytis • Orchitis