Download
1 / 21
210 likes | 407 Views
Immunisation Update for GPs 27 April 2006. Immunisation Update for Practice Nurses. Dr Peter Eizenberg

E N D
Immunisation Update for GPs 27 April 2006 Immunisation Update for Practice Nurses Dr Peter Eizenberg Director, ‘Doctors of Ivanhoe’Executive Director, North East Valley Division of General PracticeMember, Scientific Advisory Committee, NCIRSMember,NHMRC CCRE Immunisation Reference Group, RCH
General Vaccine update • Current issues in vaccination • New travel vaccines • ‘Vivaxim’ • ‘Dukoral’ • ‘Boostrix-IPV ’ • ‘VIVOTIF Oral’ • New vaccines coming soon • HPV vaccine • Herpes-Zoster vaccine • Rotavirus vaccines • Seasonal FLU & Pandemic FLU update
Australian Standard Vaccination Schedule 18 Sep 2003 ■ NIP funded from 1 Nov 2005
Current issues • Childhood IPV combination vaccines • Any dose ‘Infanrix–hexa’ requires 4th dose HIB vaccine at 12 mo (‘COMVAX’); (TAS, NSW, SA, ?some VIC) • Caution with ‘Varilrix ’ diluent • Need to reconstitute with pellet • ‘Tet Tox ’ deletion from Drs bag • 1 April 2006 • Influenza vaccine for infants 6 months to 2 years • Australia currently recommends 0.125mL dose • Two doses recommended (at least one month apart) for children aged under 9 years who are receiving influenza vaccine for the first time. • ‘Vaxigrip Junior ’ 0.25 ml syringe • ‘Pneumovax’23v PPS • single 5-yr re-vaccination for all over 65 yrs
New travel vaccines • ‘Vivaxim ’ • Hepatitis A + Typhoid • ‘Dukoral ’ • Oral Cholera vaccine (inactivated) • 2-dose schedule (for adults) • Effective against Cholera for 6 months • Effective against ETEC (Travellers Diarrhoea) for 3 months • New chapter in Handbook update to NHMRC 8th Edition AIH • ‘Boostrix-IPV ’ now available (approx $70) • or monovalent ‘IPOL’ (Sabin supply to end soon) • ‘VIVOTIF Oral’ now available (New Typhoid vaccine) • 3 doses, alt days, approx $50 • ? Other ‘new’ travel vaccines • MMR - all travellers born >Jan 1966 (if not doc’ed 2 prior doses) • Influenza - ? all travellers, all seasons, all destinations
New vaccines • Future vaccines coming soon • Human Papilloma Virus • Zoster vaccine • RSV vaccine • Rotavirus vaccine
General Vaccine update - resources • Catch-up calculator (SA Imm website)http://www.healthsa.sa.gov.au/immunisationcalculator/ • Applies to all state schedules, children up to 7 years • ‘Strive for 5’ cold-chain publication • Range 2-8 degrees C. …but STRIVE for 5 • Purpose-built vaccine fridges to replace domestic fridges • DHS newsletter April 2006 • Detailed update
Seasonal & Pandemic Flu • Issues • Seasonal FLU • Pandemic FLU • Avian FLU • Avian-mutant Influenza • Human Influenza pandemic planning
2006 Seasonal FLU • Impact of Seasonal FLU – Australia (est. annual) • Medical consults 1 million • Hospitalisations 20-40,000 • Deaths 1,500 • Days off work 1.5 million • Total economic cost $600 million • FLU Vaccination Effectiveness (during FLU season) • 70-80% effective against FLU illness • 50-60% reduction all RTIs (>65s) • 50% reduction hospitalisation, any cause (>65s) • 68% reduction death, any cause (>65s) • 40-50% reduction absenteeism during FLU season
2006 Seasonal FLU • FLU vaccine components Season 2006 • A/New Caledonia H1N1 • A/New York H3N2 • B/Malaysia • Influenza vaccine for infants 6 months to 2 years • Australia currently recommends 0.125mL dose • Two doses recommended (at least one month apart) for children aged under 9 years who are receiving influenza vaccine for the first time. • ‘Vaxigrip Junior’ 0.25 ml syringe
2006 Seasonal FLU • High-risk: age >65 yrs • 80% coverage rate (DHS supplies enough to cover 110%) • High-risk: age <65 yrs • 40% coverage rate • High-risk: Pregnancy • NHMRC recommends: vaccn during any stage of pregnancy • Normal risk (age >6 mo) • NHMRC recommends Flu vaccine for: ‘anyone who wishes to reduce their risk of FLU illness’ • Travel vaccination (age >6 mo) • all people, all destinations, all seasons
Avian FLU – Human FLU • Update on current avian FLU & Human infection • Previous FLU pandemics & future modelling • Anti-viral medications • Pandemic FLU vaccine production • What to do now (global & local) • Current Govt (C’wealth & VIC DHS) preparedness • Critical issues for GPs
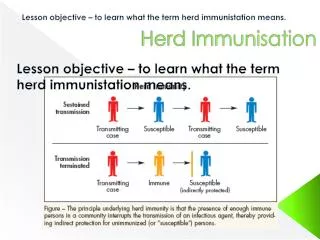
Avian FLU – Human FLU • Update on current avian FLU & Human infection • FLU causes recurrent epidemics every 1-3 yrs, for >400 years • Avian FLU vs Avian-mutant influenza • ?the next pandemic? • Human FLU types A, B, C • Birds are reservoir for type A FLU • Significant genetic variation amongst FLU strains • 15 haemagglutanins (H), 9 neurominadases (N) • Current Avian FLU H5N1 • Previous FLU Pandemics 1918, 1957, 1968 • Novel type A FLU virus with human & avian components • 1918 (H1N1) mutation from avian FLU killed 20-40 million people • 1957 – gene reassortment (H2N2) killed 1 million • 1968 – gene reassortment (H3N2) killed 1 million • Mixing of avian & human FLU genome • Requires a host with both influenzae viruses for mixing to occur
Avian FLU – Human FLU • This outbreak • Initially in birds (geese, chickens, wild birds) • Spread through migration, importing • Host range broadened to include mammals (pigs, humans) • Hong Kong outbreak 1997 (18 human cases, 6 deaths) • Dec 2003: Sth Korea chicken deaths due to Avian FLU • Dec/Jan 2004: Vietnam 10 human cases, 8 children died • 2004: also Japan, Indonesia, Thailand, Cambodia, China • 2005-6: also Azerbaijan, Iraq, Turkey • Human toll • To March 2006: total human cases 186, deaths 105 • WHO >80% infections associated with direct bird contact • NB Mortality for 1918 Spanish FLU 2.5%
Avian FLU – Human FLU • Clinical picture • Usually contact with chickens • 3 days to onset of illness • Fever, cough, SOB • Diarrhoea • Some sputum production +/- haemoptysis • Pleuritic chest pain • Lymphopenia • Thrombocytopenia • Chest infiltrate on CXR
Avian FLU – Human FLU • Computer modelling: Showsepidemic containable if: • The number of people affected <30 • The 20,000 people closest to them get prophylactic anti-virals (must be within 21 days) • Based on people infecting only 1.6 other people • If more, household quarantine may also be necessary
Avian FLU – Human FLU • Neuraminidase inhibitors • N facilitates release of virus from cells • N-inhibitors reduces release of virus & shedding from patients • Needs to be given early – before viral transmission becomes efficient • Widespread resistance to Amantadine • Possibly due to use in birds in China • Osaltamivir & Zanamivir currently being stockpiled • ? For use at site of outbreak • those at risk • Prophylaxis of contacts • Patients with confirmed disease
Avian FLU – Human FLU • Vaccines • Vaccine for birds • Vietnam 2005 20 million shots (aiming for 400 million) • Also China, Indonesia • Human vaccine: Current human vaccine against H & N proteins • A/New Caledonia H1N1; A/New York/Fujian H3N2; B/Malaysia • Humans should have human FLU vaccine • Should help prevent co-infection; reduce risk of genetic rearrangement • High risk individuals should also have Pneumovax • Human pandemic vaccine development • USA, Australia • Tested healthy under 65s – good immunity • 2 doses required • Actual strain not yet in existance
Avian FLU – Human FLU • The global approach • must assist 3rd world countries in controlling their disease • Urgency for vaccine development • Share stockpiles of vaccines & drugs • Control pandemic at source is the ideal approach • Current observations • SARS an important ‘wake-up call’ • Avian FLU spreading rapidly, but not a current threat to humans • Pandemic preparation currently rather disjointed & poorly coordinated • ‘Designated hospital’ concept provides a potentially useful organisational structure • Role of anti-virals remains unclear
FLU Pandemic planning – issues for GPs • Current surveillance expectations • DHS definition for case for suspicion • ? Is your practice appropriately prepared • Relationships/partnerships in planning? role of General Practice/Local Divisions of GP • with DHS • with regional Infectious Disease Depts • with GPDV/ADGP & C’wealth • Possible models of care, for discussion • e.g. General Practice clinics to be ‘Flu-free’ zones • Patients with Flu illness go to ‘Fever Clinics’ • Home-based care by GPs for mild Flu illnesses
FLU Pandemic planning – issues for GPs • Pandemic planning issues • Communication strategies/efficiencies • GP awareness • consistency of info, access to updates, etc • staff preparedness • Human resource/staffing issues • GP staffing of fever clinics • Equipment stock • Masks/gowns/anti-Flu medications • Anti-Flu medication prescriptions • (availability, role of Amantadine) • Practice viability/sustainability • Practice security issues