Download
1 / 23
250 likes | 506 Views
STATISTICAL ANALYSIS OF HLA AND DISEASE ASSOCIATIONS. M. Tevfik DORAK Department of Epidemiology University of Alabama at Birmingham U.S.A. (2002). http://www.dorak.info. This workshop will cover categorical data analysis for case-control design and some concepts in population genetics.

E N D
STATISTICAL ANALYSIS OF HLA AND DISEASE ASSOCIATIONS M. Tevfik DORAK Department of Epidemiology University of Alabama at Birmingham U.S.A. (2002) http://www.dorak.info BSHI 2002 Glasgow, Scotland
This workshop will cover categorical data analysis for case-control design and some concepts in population genetics AIMS Familiarization with common statistical tests useful in HLA and disease association studies Clarification of several statistical concepts Discussion of common mistakes Interpretation of results BSHI 2002 Glasgow, Scotland
Why would you do an association study? Disease gene mapping and positional cloning Molecular profiling (to predict susceptibility, outcome, response, prognosis) Basic science (to learn about disease development and subsequently to design diagnostic tests or new treatment) BSHI 2002 Glasgow, Scotland
Meaning of an association Population stratification (confounding by ethnicity) or other spurious associations Linkage disequilibrium (confounding by locus) Direct involvement in the disease process BSHI 2002 Glasgow, Scotland
Cross-validation of results Replication (population level and/or family-based) Functional studies Split the sample into two random groups (if nothing else can be done!) BSHI 2002 Glasgow, Scotland
Failure to replicate False positive in the original study False negative in the second one Population specificity Population stratification BSHI 2002 Glasgow, Scotland
Considerations at the beginning Will you have enough power? Who are the controls? Unrelated or family-based? A subgroup vs another one (males vs females)? Prospective sequential sampling or retrospective convenience samples for cases? Remember you will be testing whether the cases and controls are from the same population. The answer shouldn’t be obvious at the beginning. BSHI 2002 Glasgow, Scotland
An example of power calculation Proportion Difference Power / Sample Size Calculation (Sample sizes become 115 : 231 for P = 0.01) BSHI 2002 Glasgow, Scotland
An example of power calculation Proportion Difference Power / Sample Size Calculation http://statpages.org/proppowr.html BSHI 2002 Glasgow, Scotland
Beware of the following flaws and fallacies of epidemiologic studies confounders (known or unknown) selection bias response bias misclassification bias variable observer Hawthorne effect (changes caused by the observer in the observed values) diagnostic accuracy bias regression to the mean significance Turkey nerd of nonsignificance cohort effect ecologic fallacy Berkson bias (selection bias in hospital-based studies) SEE: http://www.dorak.info/epi/bc.html BSHI 2002 Glasgow, Scotland
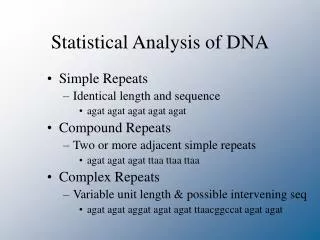
Categorical Data Analysis * 2x2 Table Analysis for Association Chi-squared (Pearson, Yates) Fisher G-test McNemar's test: TDT, HRR (Logistic Regression) * Odds Ratio - Relative Risk Difference between OR and RR Woolf-Haldane Modification Comparison of two ORs Adjusted OR * Linkage Disequilibrium Comparison of two LDs * RxC (multicontingency) Table Analysis Chi-squared G-test Exact Tests (needed for HWE) Trend Test (frequently overlooked) See http://www.dorak.info/hla/stat.html BSHI 2002 Glasgow, Scotland
The SAS System FREQ Procedure Output – I Statistic DF Value Prob Chi-Square 1 7.9047 0.0049 Likelihood Ratio Chi-Square 1 8.0067 0.0047 Continuity Adj. Chi-Square 1 7.3064 0.0069 Mantel-Haenszel Chi-Square 1 7.8840 0.0050 Phi Coefficient -0.1439 Contingency Coefficient 0.1424 Cramer's V -0.1439 * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * Fisher's Exact Test Cell (1,1) Frequency (F) 45 Left-sided Pr <= F 0.0033 Right-sided Pr >= F 0.9983 Table Probability (P) 0.0016 Two-sided Pr <= P 0.0066 BSHI 2002 Glasgow, Scotland
The SAS System FREQ Procedure Output – II Estimates of the Common Relative Risk (Row1/Row2) Type of Study Method Value 95% Confidence Limits Case-Control Mantel-Haenszel 0.5359 0.3461 0.8299 (Odds Ratio) Logit 0.5359 0.3461 0.8299 Cohort Mantel-Haenszel 0.6595 0.4892 0.8891 (Col1 Risk) Logit 0.6595 0.4892 0.8891 Cohort Mantel-Haenszel 1.2306 1.0666 1.4198 (Col2 Risk) Logit 1.2306 1.0666 1.4198 BSHI 2002 Glasgow, Scotland
Parent-Case Trios in TDT/HRR “Non-transmitted allele” “control” □ ○ □ □ ○ ○ BC AB AB CD AC BD ● ● ■ □ ○ BB BC AB AC BB ■ “transmitted allele“ “case” BC BSHI 2002 Glasgow, Scotland
- AN EXAMPLE OF TDT - TRANSMISSION DISEQUILIBRIUM OF HLA-B62 TO THE PATIENTS WITH CHILDHOOD AML (Dorak et al, BSHI 2002) Out of 13 parents heterozygote for B62, 12 transmitted B62 to the affected child and 1 did not McNemar’s test results: P = 0.0055 (with continuity correction) odds ratio = 12.0, 95% CI = 1.8 to 513 BSHI 2002 Glasgow, Scotland
Multiple comparisons Not needed if the study is not hypothesis driven (i.e., a fishing experiment) Not needed if the study is hypothesis driven ('Possible relevance of the HLA system' is not a valid hypothesis in this context. Those studies belong to the fishing experiments group) Therefore, it is not clear when it is needed in HLA association studies. Most frequently, it is an excuse for a busy reviewer to avoid a comprehensive review Best solution is to avoid facing this problem -ideally by replication and/or functional data to support the statistical association before it is dismissed as a spurious result of multiple comparisons BSHI 2002 Glasgow, Scotland
Common Mistakes in Statistical Evaluation of Association Study Results - I Confusion between corrections (Yates/Williams for continuity VS Bonferroni) Confusion between RR and OR (they are not the same) Confusion between expected and observed values in cells of a contingency table Small sample size issue Don’t confuse a negative result with lack of power (‘No significant difference between the two groups and they were pooled’ VS ‘the difference did not reach significance due to small sample size’ are different interpretations of the same phenomenon, i.e., lack of power) Using Chi-squared test for small sample size (why not use Fisher all the time?) Using Chi-squared test for HWE (use exact test or G-test) BSHI 2002 Glasgow, Scotland
Common Mistakes in Statistical Evaluation of Association Study Results - II One-tailed and two-tailed P values (always use two-tailed) Trend test for a multicontingency table? (if appropriate, more powerful) Multiple comparison issue Failure to give the strength of the association (OR, RR, RH) Use of the word ‘proof’. Does statistics prove anything? (A ‘P value’ provides a sense of the strength of the evidence for or against the null hypothesis of no association) Reliance on large sample effect to achieve significance Showing P values as 0.000 (this means P < 0.001) Confusion between association and linkage BSHI 2002 Glasgow, Scotland
Association and Causality? However strong an association does not necessarily mean causation. Several criteria have been proposed to assess the role of an associated marker in causation. Some of those are as follows: 1. Biological plausibility 2. Strength of association (this is not measured by the P value) 3. Dose response (are heterozygotes intermediate between the two homozygotes, or is homozygosity showing a stronger association than just having the marker?) 4. Time sequence (this is inherent in the germ-line nature of HLA genes) 5. Consistency (next slide lists reasons for inconsistency in HLA association studies) 6. Specificity of the association to the disease studied BSHI 2002 Glasgow, Scotland
Why Are the Inconsistencies? (I) 1. Mistakes in genotyping (lack of HWE in controls is usually an indication of problems with typing rather than selection, admixture, nonrandom mating or other reasons of departure from HWE) 2. Poor control selection (would your controls be in the case group if they had the disease, and would the cases be in your control group if they were free of the disease?) 3. Design problems including the statistical power issue (negative results due to lack of statistical power should be distinguished from truly negative results observed despite having sufficient power) 4. Publication bias (are there many more studies with negative results but we have never heard about them?) 5. Disease misclassification or misclassification bias BSHI 2002 Glasgow, Scotland
Why Are the Inconsistencies? (II) 6. Excessive type I errors (are the positive results due to using P < 0.05 as the statistical significance?) 7. Posthoc and subgroup analysis (are positive results due to fishing (data dredging)?) 8. Unjustified multiple comparisons and subsequent type II error 9. Failure to consider the mode of inheritance in a genetic disease 10. Failure to account for the LD structure of the gene (only haplotype-tagging markers will show the association, other markers within the same gene may fail to show an association and generate background noise) 11. Likelihood that the gene studied account for a small proportion of the variability in risk BSHI 2002 Glasgow, Scotland
Further Information Select ‘Biostatistics' or ‘Epidemiology’ at http://www.dorak.info or write to me at dorakmt:at: lycos.com [please do not add to your address book as it will change periodically] BSHI 2002 Glasgow, Scotland
I am grateful to the BSHI Organizing Committee for giving me the opportunity to run this workshop at BSHI 2002 in Glasgow. I particularly thank Nancy Henderson and Ian Galbraith also for their hospitality. BSHI AGM 5:15 pm All members should attend BSHI 2002 Glasgow, Scotland