Download
1 / 16
230 likes | 733 Views
A Case of Leptospirosis Problems in Lab diagnosis. Presented by Dr.B.KrishnaKumar Post Graduate in Medicine Prof. Dr.S. ShivaKumar’s Unit Stanley Medical College.

E N D
A Case of LeptospirosisProblems in Lab diagnosis Presented by Dr.B.KrishnaKumar Post Graduate in Medicine Prof. Dr.S. ShivaKumar’s UnitStanley Medical College.
A 19 year old male presented with C/o Fever Body ache past 7 days. Headache High coloured urine
Presenting illness • C/o Fever-high grade, intermittent associated with chills & rigors • H/o Headache & retroorbital pain • H/o Cough with minimal blood streaked sputum • H/o Severe myalgia – 1 week duration • H/o High coloured urine • H/o Epistaxis +
Past History • Not or known HT/DM/PT • No previous H/o Jaundice • Personal History – Nothing significant • Family History – Nothing significant
Occupational History • Patient hailing from a village near Ambur town but working as fitter in Ambattur. Daily he uses to go his native place and walk with barefoot. • H/o contact (regular) with stagnant water in the street during rainy season.
Vital signs: Pulse Rate : 96 / min BP : 100/70 mm Hg RR : 20 / min • General Examination Pt. • Consious • Oriented • Febrile + • Icterus + • Conjuctival suffusion / Sub conjuctival hemorrhage in left eye • Muscle tenderness + • Not anaemic • No cyanosis • No generalized lymph node enlargement • No pedal edema
System Examination • CVS - NAD • RS - NAD • ABDOMEN - Soft, BS+ Liver + 4cm below RCM • CNS - NFND
Lab Investigations Blood urea - 43 mg% Blood Sugar -108 mg% S.creatinine - 0.8mg% S.Electrolytes Na+ 129 mEq/L K+ 4.1 mEq/L Urine Albumin - nil Sugar - nil Deposit 2-3 deposits Bl.TC-9000 cells/cumm DC - P 70 L 26 E 4 ESR - 25 / 42 mm/hr Hb% -10.2 gms Platelets -1.9 lakhs MP/MF-Negative WIDAL –Negative
Peripheral smear – Microcytic hypochromic Reticulocyte 1% • LFT • Bilirubin • Total 4.6 mg% • Direct 3.2 mg% • SGOT 96 IU/L • SGPT 124 IU/L • BT - 3 mins • CT - 6 mins • HBSAg - Negative
MSAT Ictero 1:40 Patoc 1:160
Diagnosis • During rainy season,19 years old male presented with • Fever, myalgia, conj.suffusion, subconjuctival hamhge , ICTERUS – 1 week duration • Clinical features - Suggestive of Leptospirosis • MSAT Negative in First sample - 10th day. • Became Positive only on 12th day. • But MAT – Negative till 20 days • Third sample only - Positive.
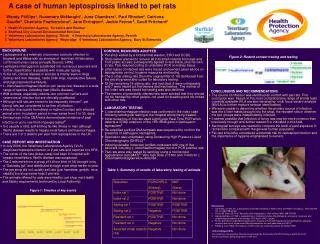
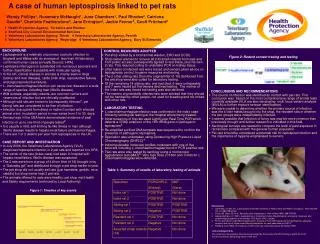
American Journal of clinical microbiology- Brazil 1998Angelo P.Brendo et al.Summary (108 samples) • Slide Agglutination test (SAT) • 65% positive in first sample • 94% positive in second sample. • Mat • 40 % positive in first sample. • SAT/ MAT
MAT 108 • 46 samples +ve • 62 samples -ve • SAT 108 • 70 samples +ve ( 22% ) • 48 samples -ve • Advantages of SAT • Rapid screening test for current diagnosis. • MAT – Time consuming /required specialized personnel. (More than 30samples/day) • Persistent antibodies in MAT interfere with current diagnosis • MSAT/ELISA Igm – Rapid Screening Tests
Problems in practice • < 6 days – Diagnostic test not available • Therefore clinical diagnosis adequate to start treatment. • Always confirm diagnosis after 6 days. • If the first sample is –ve repeat the tests after few days • SAT/ELISA are the tests of choice for current infection.
Interpretation of Tests 0 1 week 1 month 2 months 1 yr 5 yrs SAT/ELISA MAT