Download
1 / 44
440 likes | 470 Views
Explore the causes and effects of vascular diseases, including atherosclerosis, aneurysms, and arteriovenous fistulas. Learn about the anatomy of blood vessels and the pathogenesis of atherosclerosis. Discover how vascular pathology impacts human health.

E N D
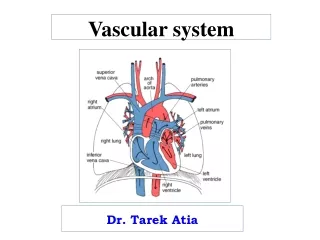
Pathology of vascular system د هبة احمد غيدان Lec. 1
Vascular disorders are responsible for more morbidity and mortality than any other category of human disease. Although the most clinically significant lesions typically involve arteries, venous diseases also occur. • Vascular pathology results in disease via three principal mechanisms: 1. Progressive narrowing of the lumen associated with progressive ischemia of the relevant tissues. 2. Thrombosis associated with partial or complete luminal obstruction and/or embolism. 3. Aneurysmal dilatation that may eventuate in rupture with ischemic and destructive consequences
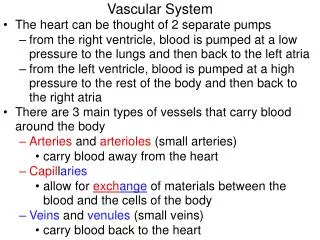
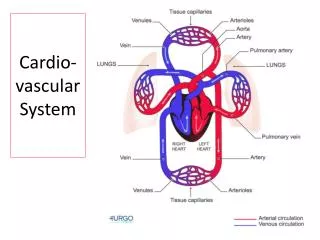
Normal anatomy & Histology: Basic components of the wall of blood vessels are including; 1. Endothelial Cells (ECs) & Smooth Muscle Cells (SMCs). 2. Extracellular Matrix (ECM). These components are arranged into three layers: (from lumen to outside) Intima:consist of single layer of endothelial cells. Media: consist of smooth muscle cells. Adventitia: Consist of connective tissue, VasaVasorum & nerve fibers.
According to their size & structure, arteries can be classified into the followings: 1. Large, elastic arteries: Example: Aorta & its branches (like subclavian, common carotid, iliac, & pulmonary arteries), Have elastic fiber rich media (expand during systole & recoil during diastole 2. Medium size arteries (muscular arteries): Like coronary, renal arteries .Their media is composed predominantly of SMC, which regulate regional blood flow & blood pressure by change the size of lumen by vasoconstriction & vasodilatation. 3. Small arteries & Arterioles : Their media consist of smooth muscles contraction cause changes in diameter that regulates systemic arterial blood pressure, (as much as small vessel, the higher resistance & pressure). So the arterioles are the principals points of physiologic resistance (control the blood pressure).
Congenital Anomalies 1- Berry aneurysmsoccur in cerebral vessels; when ruptured these can cause fatal intracerebral hemorrhage. 2- Arteriovenous fistulas : They are abnormal, typically small, direct connections between arteries and veins that bypass the intervening capillaries. Complications: • Ruptured and cause sever hemorrhage (e.gintracerebral hemorrhage). • Large arteriovenous fistulas become clinically significant by shunting blood from the arterial to the venous circulations and forcing the heart to pump additional volume; high-output cardiac failure.
Berry aneurysm Congenital defect in the media of vessels of circle of willis
ARTERIOSCLEROSIS This generic term refers to a group of disorders having in common thickening and loss of elasticity of arterial walls and thus leading to sclerosis i.e. hardening of the wall. Under this heading come three distinctive morphological variants, namely: 1. Atherosclerosis,the most frequent & important form. 2. Monckeberg medial calcific sclerosis, 3. Arteriolosclerosis: (Disease of small arteries & arterioles). Most often in patient withhypertension & diabetes mellitus.
ATHEROSCLEROSIS This disease is responsible for more deaths and serious complications than any other disorder. This is because its prime targets are vital arteries, namely the coronaries, cerebral arteries, & the aorta so its major consequences are : 1. Myocardial infarction (alone responsible for about 25% of all deaths) 2. Cerebral infarction 3. Aortic aneurysm
ATHEROSCLEROSIS is“a disease primarily of large elastic arteries and medium sized muscular arteries. Its basic lesion is the atheroma. • Atheroma (fibro-fatty plaque) is a raised patch within the intima having a core of lipid (mainly cholesterol and its esters) and a cap of fibrous tissue”.
Pathogenesis of atherosclerosis • The most widely accepted theory of pathogenesis is called the response to injury hypothesis. This theory states that : • Lesions of atherosclerosis are initiated as a response to some form of repeated chronic injury to arterial endothelium. • This injury increases endothelial permeability to plasma lipids as well as permitting blood monocytes and platelets to adhere to the endothelium. • Monocytes subsequently enter the intima, transform into macrophages and accumulate lipids to become foam cells. • Factors released from both platelets and macrophages cause migration of smooth muscle cells from the media into the intima with eventual synthesis and accumulation of collagen.
Macrophages produce, among other substances, toxic free oxygen radicals (ROS) that oxidize (modify) LDL in the lesions. This oxidized LDL is considered atherogenic, as it is • Chemotactic to blood monocytes • Inhibits macrophage motility thus preventing them from leaving the atheroma. • Cytotoxic to endothelial cells increasing their permeability • This suggests that antioxidants e.g. vitamin E and ß-carotene may be effective in preventing atherosclerosis by reducing LDL oxidation.
Risk factors of atherosclerosis : • Risk factors of atherosclerosis are expressed largely in terms of the incidence of deaths caused by ischemic heart disease (IHD). • This is because atherosclerosis does not by itself produce signs and symptoms but its prevalence is detected by its effects on the most commonly involved arteries which are the coronaries.
Risk factors that predispose to atherosclerosis and the resultant IHD can be divided into two main groups Major A. Potentially modifiable (controllable) 1. Diet and hyperlipidemia 2. Hypertension 3. Cigarette smoking 4. Diabetes mellitus B. Non modifiable 1. Increasing age 2. Male gender 3. Family history 4. Genetic abnormalities
Minor (uncertain risks) 1. Obesity 2. Physical inactivity 3. Stress (type A personality) 4. High carbohydrate intake 5. Lipoprotein (a) 6. Hardened unsaturated fat intake 7. Chlamydia pneumonia 8. Hyperhomocystinemia
Pathlogical features of Atherosclerosis: Pathology of atherosclerosis passes in three stages: 1- Fatty streaks: 2. Atheromatous Plaques: 3. Advanced atheromatous lesions:
1- Fatty streaks: characterized by intimal thickening & lipid accumulation, this is the precursor of atheromas. Components of Fatty streaks: These streaks are composed of lipid laden foam cells. it appear in Aorta of children below 10 years, regardless the sex, race, geography, environment (not all streaks are tend to become plaques). Gross: multiple yellow, fat spots (fatty dots) less than 1mm in diameter that coalesce into large streaks of 1cm or more.
Atheromatous Plaques: These are raised focal lesions within the intima, also called (Fibrofatty or Fibrolipid Plaques). These plaques consist of two parts: Caps: composed of SMC & dense collagen fibers, beneath & the sides of cap, there are cells include (T-lymphocytes, Macrophages, & SMC). Core: consist of I. disorganized mass of lipid (cholesterol & cholesterol esters). II. Cholesterol clefts. III. Foam cells, they are tissue macrophages filled with lipid (called lipid laden cells), Sometime, SMC are also form lipid laden cells. IV. Neovascularization: formation of new blood vessels at the periphery of Atheromatous lesions . These plaques are varied in their size from 0.3 to 1.5cm in diameter, sometimes they are coalesces to form large masses protrude into lumen.
3. Advanced atheromatous lesions: These lesions are called eccentric lesions (partial, patchy lesions), as disease become advanced, these lesions becomediffusely involved the The basic lesion in atherosclerosis is a focal intimal thickening termed atheromatous plaque or fibro-fatty plaque. Each plaque is white to whitish yellow elevation up to 1.5 cm in diameter; adjacent plaques, however, may fuse to form larger plaques.
The coronary artery shown here has narrowing of its lumen due to build up of atherosclerotic plaque
There is a severe degree of narrowing in this coronary artery. It is "complex" in that there is a large area of calcification on the lower right, which appears bluish on this H&E stain. Complex atheroma have calcification, thrombosis, or hemorrhage.
Stages of ATH Stage 1: Fatty streaks (arrow) within the aorta
The major components of a well-developed intimalatheromatous plaque overlying an intact media.
This high magnification of the atheroma shows numerous foam cellsand an occasional cholesterol cleft. A few dark blue inflammatory cells (lymphocytes) are scattered within the atheroma.
This is mild coronary atherosclerosis. A few scattered yellow lipid plaques are seen on the intimal surface of the opened coronary artery traversing the epicardial surface of a heart.
These three aortas demonstrate mild, moderate, and severe atherosclerosis from bottom to top. At the bottom, the mild atherosclerosis shows only scattered lipid plaques. The aorta in the middle shows many more larger plaques.
Atherosclerosis, microscopicThis high-magnification view of the necroti center of an aortic atheroma shows foam cells and cholesterol clefts
The most heavily involved arteries by atherosclerosis and in descending order are 1. Abdominal aorta 2. Coronaries 3. Popliteal arteries 4. Descending thoracic aorta 5. Internal carotid arteries 6. Arteries forming the circle of Willis at the base of the brain. Atheromatous plaques are patchy in distribution and may involve the arterial wall in asymmetrical fashion i.e. involve one portion of the wall circumference more severely than elsewhere and as such produce eccentric lesions.
Complicationsofatherosclderotic lesions : 1. Focal rupture, ulceration, & erosion of the luminal surface of Atheromatous plaques. These changes induce thrombus formation, or result in discharge of contents of atheromatous lesion into the circulation, called (cholesterol emboli). 2. Hemorrhage: Hemorrhage into the plaques (mainly in coronary arteries), may result in formation of Hematoma within the plaques that increase the risk of rupture. 3. Superimposed thrombosis: This is a most feared complication; usually follow the rupture, ulceration, & erosion of luminal surface of plaque. 4. Embolization:it is a complication of superimposed thrombosis. 5. Aneurysmaldilatation:Weakening in the wall of involved vessels, result in abnormal dilatation in the wall of blood vessel. 6.Calcification, this may be patchy or massive.
Atherosclerosis, gross This coronary artery opened longitudinally shows yellowish atheromatous plaques over much of its intimal surface. There is focal hemorrhage into a plaque, a complication of atherosclerosis that can acutely narrow the lumen
Complications of ATH: Bleeding within atheromatous lesion
CONSEQUENCES OF ATHEROSCLEROTIC DISEASE The principal outcomes depend on the size of the involved vessels, the relative stability of the plaque itself, and the degree of degeneration of the underlying arterial wall: Smaller vessels can become occluded, compromising distal tissue perfusion. Ruptured plaque can embolize atherosclerotic debris and cause distal vessel obstruction, or can lead to acute (and frequently catastrophic) vascular thrombosis. Destruction of the underlying vessel wall can lead to aneurysm formation, with secondary rupture and/or thrombosis.
In smaller arteries such as the coronary, cerebral, popliteal, renal and mesenteric arteries, the main effect is narrowing of the lumen leading to chronic ischemia. However, if this is complicated by superadded thrombosis or hemorrhage in to the plaque, occlusion of the vessel lumen occurs with subsequent catastrophic events such as myocardial infarction, cerebral infarction, gangrene of lower limbs, renal or intestinal infarctions.
In large arteries such as the aorta the main complications are 1. Development of large mural thrombi over the plaques that may dislodge leading to peripheral emboli. 2. Aneurysmal dilatation of the wall due to weakness of the media. 3. Rupture of the atheroma leading to the development of cholesterol emboli.
MEDIAL CALCIFIC SCLEROSIS (Monckeberg’s arteriosclerosis) This variant of arteriosclerosis is of undetermined etiology & is characterized by ring-like calcifications within the media of medium sized to small muscular arteries. The calcification does not narrow the lumen and thus the condition is of little clinical significance. It may coexist with atherosclerosis in the same artery. The arteries most commonly affected are those of the extremities (femoral, tibial, radial and ulnar), and those of the genital tract in both sexes. The condition can be demonstrated in individuals over the age of 50 years