Download
1 / 115
1.3k likes | 2.04k Views
Growth (Short Stature, Obesity) Diabetes Mellitus in Children. Sioksoan Chan-Cua, MD Associate Professor Pediatric Endocrinologist. Learning Outcomes. Short stature Identify causes of short stature Acquire skill in history-taking, physical examination in a child with short stature

E N D
Growth (Short Stature, Obesity)Diabetes Mellitus in Children Sioksoan Chan-Cua, MD Associate Professor Pediatric Endocrinologist
Learning Outcomes Short stature • Identify causes of short stature • Acquire skill in history-taking, physical examination in a child with short stature • Diagnose pathologic short stature • Propose diagnostic work-ups • Provide treatment plan
Growth - Height • Normal growth • Short stature • Causes • Diagnosis • history and physical examination • work-up • treatment / management plan
Growth Rate Through Adolescence At birth, full-term baby’s Length: 50 cm (20 in ) Weight: 3 kg (7 lb) Birth to 1 year: 18 - 25 cm (7 - 10 inches ) 1 to 2 years: 10 to 13 cm (4 to 5 inches) 2 years to pre-puberty : 5 to 6 cm (2 to 2.5 inches) Puberty: • Girls (11 yr) 6 - 11 cm 2.5 - 4.5 in • Boys (13 yr) 7 - 13 cm 3 - 5 in
DEFINITIONS • SHORT STATURE • Height < 3rd percentile for age • GROWTH FAILURE • Growth rate < 5 cm/year after age 2 years Short Stature with Slow Growth Rate
Factors Affecting Growth • Nutrition (malnutrition) • Diseases (chronic diseases) • Genes/ heredity • Hormones • Psychological factors
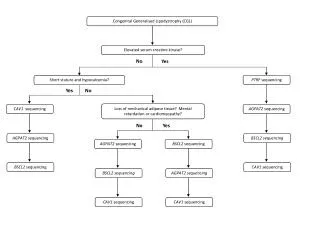
Genetic Control of Growth • Chromosomes • Abnormalities – missing, or trisomy • Genes • normal development & function of the pituitary • growth hormone / insulin-like growth factor axis • Mutations of these genes • responsible for abnormal growth • Growth hormone deficiency • GHD IA: AR, complete GH-1 gene deletion • GHD IB: AR, point mutation • GHD II: AD • GHD III: x-linked inheritance
Play a role in determination of pituitary cell lineages Pituitary-specific transcription factors
Hormones Affecting Growth • Growth hormone (GH) • Thyroid hormone • Glucocorticoids • Sex hormones • Insulin – important fetal growth factor (infant of diabetic mother is macrosomic)
Hormonal Control of GrowthPituitary Gland and GH GH is a protein with 191 amino acids and its secretion is pulsatile. GH may be influenced by ghrelin levels in the hypothalamic-pituitary portal circulation and the systemic circulation
FAMILIAL SHORT STATURE • Growth may be reduced between 6 & 18 months then growth becomes steady but below the 5th P • No weight deficits for height and no bone age delay (BA = CA) • TREATMENT: • None • Long term GH results in very modest height increase
CONSTITUTIONAL GROWTH DELAY • A common cause of short stature & sexual infantilism in the adolescent • Normal growth progression paralleling a lower percentile curve until catch up growth occurs • Usually occurs in boys; occurs occasionally in girls • (+) family history • TREATMENT: • Reassurance • Testosterone only if BA > 12 years for 4-6 months
CAUSES of SHORT STATURE PATHOLOGICAL • Disproportionate • Bone development disorders (Skeletal dysplasia) • Achondroplasia • Rickets • Other skeletal disorders
CAUSES of SHORT STATURE PATHOLOGICAL • Proportionate • Chromosome defects • Endocrine disorders • Low birth weight short stature (IUGR) • Nutritional deficiency • Chronic systemic disease • Psychosocial deprivation
Chromosomal Abnormality • Somatic • Down syndrome • Sex chromosome • Turner syndrome • Short stature (< 144cm) • Gonadal dysgenesis • Skeletal deformity • Cubitus valgus • Short metacarpals
Prader-Willi Syndrome • Obesity - hyperphagia • Moderate mental retardation • Short stature • Hypogonadism • Small hands and feet • Facies with narrow bifrontal diameter, almond eyes, full cheeks
Russell-Silver Syndrome • Intrauterine growth retardation • Postnatal short stature • Small triangular facies • Limb asymmetry
Endocrine Causes of Short Stature • Hypopituitarism - GH deficiency (GHD) • Hypothyroidism • Hypercortisolism • Hypogonadism
PITUITARY DWARFISM • PRIMARY PITUITARY DISEASE • Pituitary hormone deficiency • Intrasellar tumor • Other destructive processes (infection, trauma) Short stature secondary to hypopituitarism is due to lack of stimulation of growth of long bone
CHARACTERISTICS OF GHD • Diminished growth rate • Delayed bone age • GH (<10 μg/L) • Growth response to treatment with hGH EARLY CLUES TO GH DEFICIENCY • Hypoglycemia • Micropenis • Facial midline malformation • Neonatal injury
Hypothyroidism • Hypothyroidism → short stature • Congenital • Acquired
Congenital Hypothyroidism History • Autoimmune thyroid disease in the family • Intake of anti-thyroid medication in the mother • Familial congenital hypothyroidism • Presence of congenital hypothyroidism associated with deafness and goiter • Prolonged jaundice in the neonate • Poor suck in the neonate • Poor cry in the neonate • Constipation in the neonate
Congenital Hypothyroidism PE • Hypothermia • Mottled, dry, coarse skin • Jaundice • Large fontanelle • Macroglossia • Hoarse cry • Distended abdomen • Umbilical hernia • Hypotonia • Goiter
Hypercortisolism – Cushing syndrome • Excessive cortisol • Short and obese • Causes: • Endogenous: tumor • Exogenous: prolonged steroid intake
Abnormal levels of Sex Hormone Hypogonadism- • both growth and sexual development may be retarded Turner syndrome • insufficient amounts of the female sex hormone, estrogen • delays in growth and sexual development • Precocious puberty • Early growth spurt and premature closure of epiphyses • Adult height: Short
HISTORY • Birth weight & birth length • Previous height and weight data (growth velocity) • Time of adolescent development • Dietary history • Past Illnesses • School performance • Family patterns of growth • the heights of parents, grandparents, siblings, and other close relatives • any history of early or late puberty (growth spurt and sexual development) in family members
Physical Examination • Height • Weight • Arm span • Upper & lower body segment • Dysmorphic features • Associated anomalies
Work-ups • X-ray for bone age • Imaging – CT scan / MRI of sella • Blood tests: • Blood chemistry • Chromosomal analysis • Hormonal stimulation tests Bone age delayed compared to chronological age in GHD and hypothyroidism
Blood Tests • Blood tests • BUN, Cr, Ca, P, alk phosphatase, SGPT • TSH, T4 • Cortisol • insulin-like growth factor I (IGF-I) • Chromosomal analysis • Tests for GH SecretionGH Stimulation tests • GH<10 μg/L
Treatment of Short Stature • Depends on etiology • Hypothyroidism: levothyroxine • Growth hormone deficiency: GH • Cushing syndrome • Tumor removal • Adjust dosage of steroid • Turner syndrome/ Prader Willi syndrome: GH • Achondroplasia: limb lengthening
Indications of GH Use in Children • Growth hormone deficiency • Turner syndrome • Small for gestational age (not catching up in height) • Prader-Willi syndrome • Chronic renal insufficiency • Idiopathic short stature – • expected to grow shorter than • 5’3” for boys • 4’11” for girls
PHYSIOLOGIC EFFECTS OF GH • Short-term administration of GH promotes • Lipolysis • loss of visceral adipose tissue - the most dramatic metabolic effect of GH • stimulates protein synthesis • increases lean body mass • stimulates bone turnover • causes insulin antagonism • alters total body water
Summary • Normal growth • Growth velocity • Factors affecting growth • Short stature • “normal” variants • Pathological short stature needs evaluation • History, PE • Treatment depends on etiology • GH therapy is approved in some conditions
Childhood Obesity Sept,2, 2009
Learning Outcomes Obesity • Identify causes of obesity • Acquire skill in history-taking, physical examination in a child with obesity • Use growth charts and BMI charts • Propose diagnostic work-ups • Provide treatment plan
Childhood Obesity • Definition • Epidemiology • Physiology • Causes • Evaluation • Treatment
Definition of Overweight and Obesity Barlow SE and the Expert Committee. Expert committee recommendations regarding the prevention, assessment, and treatment of child and adolescent overweight and obesity: Summary report. Pediatrics. 2007;120;S164-S192.
Growth (Height and Weight ) Charts CDC Measurements of weight and height. Plot data on the growth charts. OK135S057
Body Mass Index (BMI) BMI = Weight (kg) Height (m2) BMI charts – examples: CDC, WHO
In children, BMI is age and gender specific BMI percentile can be used to identify childhood obesity Obesity 95th P 85th P Overweight http://www.cdc.gov/nchs/about/major/nhanes/growthcharts/charts.htm OK135S060
WHO BMI Cut-offs • Overweight: > +1SD (= =BMI 25 kg/m2 at 19 years) • Obesity: > +2SD (= BMI 30 kg/m2 at 19 years) • Thinness: < -2SD • Severe thinness: < -3SD
Obesity Overweight Normal Thinness Severe Thinness
Epidemiology Prevalence of overweight and obesity • Of the world’s children and adolescents aged 5 -17 years, about 10% estimated to be overweight among them, 1/4 obese (30-40 million) Report of the International Obesity Task Force to the WHO.Obesity Reviews, 2004 Globally, generally there is 2-3 x ↑ Lancet 2002; 360:474
Epidemiology In the Philippines, 7th National Nutrition Survey (FNRI): Prevalence of overweight • 2.0% among 0-5 years-old children • 1.6% among 6-10 years-old children • 4.6% among 11-19 year-old adolescents
80% 60% 40% 20% 0% <5th 5th-84th 85-94th ≥95th Prevalence of overweight and obesity Among 2022 adolescents (10-19 years) in private and public schools, Metro Manila (2007-2008) • 13% overweight (BMI 85-94th P) • 8% obesity (BMI ≥95th P) Cua S. 2008
Study (S Cua, 2008):Adolescents (n=2022; age: 11-18 yr) from 6 high schools (3 private, 3 public) The prevalence of overweight about 3-fold higher in the private school students The prevalence of obesity: 5-fold higher in the private school students
Prevalence of overweight among students was higher in Private Schools in Metro Mla • R. Florentino, et al, (2002) • 1208 male and female students, aged 8-10 yr • the prevalence of overweight (BMI ≥ 95th P) among private school children was almost 4 x higher than those in public school