Download
1 / 18
200 likes | 431 Views
VITAMIN D and Pathologies. vitamin D 2 (diet). 25-hydroxylase. 1 a -hydroxylase. Tightly regulated. Synthesis of active vitamin D. 10% ,. 90% ,. Bile Salts. calcidiol. 1,25(OH) 2 D 3 calcitriol. Vitamin D pathway Cholesterol 7-dehydrocholesterol UVB rays (skin)

E N D
vitamin D2 (diet) 25-hydroxylase 1a-hydroxylase Tightly regulated Synthesis of active vitamin D 10%, 90%, BileSalts calcidiol 1,25(OH)2D3 calcitriol
Vitamin D pathway Cholesterol 7-dehydrocholesterol UVB rays (skin) Inactive Vit D3 (cholecalciferol) 25 hydroxylase (liver) Calcidiol (25-hydroxycholecalciferol) 1α-hydroxylase (kidney) Calcitriol (1,25-dihydroxycholecalciferol) Active Vitamin D
Hypercalcaemiavs Hypocalcaemia • Symptoms • Hypercalcaemia • neuromuscular irritability • muscle cramps/tetany • Seizures • Hypercalcaemia • nausea/vomiting/constipation/anorexia • tiredness, confusion, depression, headaches • muscle weakness • kidney stones/ectopic calcification • loss of bone • polyuria/polydipsia
Treatment for hyper/hypocalcaemia • Hypercalcaemia (>3-3.5mmol/l must treat as emergency) • fluids (normal saline) • loop diuretic (furosemide) • calcitonin • bisphosphonates • oral phosphate • long term ? parathyroid gland surgery • Hypocalcaemia • acute (neuromuscular symptoms) • IV calcium gluconate • chronic • oral calcium • vitamin D (form will depend on where the defect is)
What is tetany? Tetany– as E.C. [Ca2+] falls, peripheral nerve fibres discharge spontaneously, leading to muscle contractions • Freq observed in the wrist, pulled into flexed position • carpopedal spasm
What do they look like on an ECG? Normal Hypocalcaemia Hypercalcaemia
Renal osteodystrophy – aka renal bone disease • Variety of metabolic bone diseases • High turnover • Osteitisfibrosa • Low turnover • Osteomalacia • Adynamic bone disease • Amyloidosis
Osteitisfibrosa(2o hyperparathyroidism) • High rate of turnover associated with persistently high PTH • 2o hyperparathyroidism • Increased bone resorption • Increased number/activity OB and OC • Increased Howship’s lacunae (resorption pits) • Deposition of fibrous tissue • As bone turnover rapid they make disorganized, woven type bone, no strength (similar to that of Paget’s)
Osteomalacia • similar to Rickets but in adults • Don’t have high PTH (often low/normal) • Low rate bone formation (undetectable) and turnover • Bone doesn’t buffer Ca2+ well – effectively locked in bone
Adynamic bone disease • – nothing happening to bone, static • Becoming most common form of renal bone disease • Normal/decreased osteoid • No tissue fibrosis • Decreased osteoblasts and osteoclasts • Low or unmeasurable rates of bone formation • >50% dialysis patients • More commoin in DM/ESRF • Hard to distinguish from OP • Are patients old/postmenopausal? • Symptomatic control, can’t cure
Amyloidosis • Deposition of β2-microglobulin • Takes 7-10 years to develop; not a problem for diabetics, often die before this develops
Low calcium Calcium regulation Hyperparathyroidism 1ry – extra secretion of PTH Negative feedback 2ry – kidney disease: reduced active Vit D production Reabsorb bone PTH In mitochondria Activate Vit D Absorb more from gut In tubules: reabsorb calcium 3ry – after chronic high PTH levels, PT glands become desensitised and produce constitutively high levels of PTH High calcium
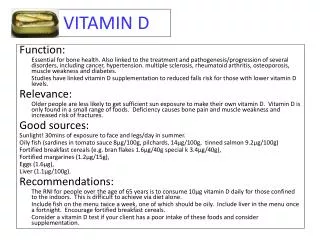
↓Vitamin D metabolism or action = • Reduced bone matrix mineralisation. • Deficiency of Vit D (sunlight, diet)/ Malabsorption (egcoeliac’s)/ Renal disease (eg CRF) • Rickets (children) • Bow legs • Deformities of ribcage, long bones and spine • Osteomalacia (adults) • Bone pain • Pathological fractures • Waddling gait (prox myopathy) • Investigations • Bloods - ↑Alkaline Phosphatase (due to increased osteoblastic activity) • x-ray – may show some changes (demineralisation) • Treatments • Vitamin D supplements depending on what the condition is. Calcitriol supplements should only be given to patients with chronic renal failure. If the cause is dietary deficiency or inadequate sunlight exposure then these can be treated without medication.
Hyperparathyroidism • 1o hyperparathyroidism • Affects PTH gland directly • 90% of all hypercalcaemia • Often due to a tumour • High plasma Ca2+
2o hyperparathyroidism • Vitamin D deficiency – usually renal disease • Low plasma Ca2+ (hypocalcaemia) - stimulates PTH production from glands • No increase in vitamin D production, no increase in Ca2+ absorption, no –ve feedback on parathyroids • Sustained PTH secretion • PTH can only act on bone • Ca2+ loss from bone • Renal bone disease
3o hyperparathyroidism • Long-term problem associated with renal failure • PTH glands become desensitised to Ca2+ and vitamin D (lose receptors); no negative feedback • Even if Ca2+ and vitamin D levels corrected PTH still produced • Glands often hyperplastic • High plasma Ca2+
Vascular calcification In dialysis patients • Calcium not deposited in bone • Instead is deposited with hydroxyapatite in blood vessels causing calcification • Often seen in coronary arteries and in x-rays without angiography • Within 1 year of dialysis, have BVs of an 80 year old due to calcification