Download
1 / 177
1.83k likes | 2.27k Views
Parasitology/ Helminths (3 hours). 1. Defines “ Helminth ’’ 1.1 Lists the helmints classification. 1.2. Defines the structure of helminths 1.3. Defines the life cyles of helminths ; lists the egg and larva structures.

E N D
Parasitology/Helminths (3 hours) • 1. Defines “Helminth’’ • 1.1 Lists the helmints classification. • 1.2. Defines the structure of helminths • 1.3. Defines the life cyles of helminths; lists the egg and larva structures. • 2. Lists the clinical tables related with helminths and defines pathogenetic mechanisms. • 2.1. Defines the clinical importance of helminths. • 2.2. Defines the sample taking related with infections of helminths. • 2.3. Lists the laboratory diagnostic methods.
Nematodes • Ascaris lumbricoides • Dracunculus medinensis • Enterobius vermicularis • Wuchereria bacrofti • Ancylostoma duodenale • Toxocara spp. • Loa loa • Strongyloides stercoralis • Trichinella spiralis • Trichuris trichiura
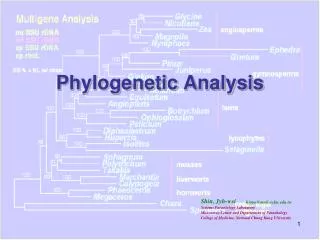
Helminths • Helminth is a general term for a parasitic worm. • The helminths include • the Platyhelminthes or flatworms (flukes and tapeworms) • the Nematoda or roundworms.
Helminths • all helminths are relatively large (> 1 mm long); • some are very large (> 1 m long). • all have well-developed organ systems and most are active feeders. • the body is either flattened and covered with plasma membrane (flatworms) • or cylindrical and covered with cuticle (roundworms). • some helminths are hermaphrodites; • others have separate sexes.
Helminths • Helminths are worldwide in distribution; infection is most common and most serious in poor countries. • The distribution of these diseases is determined by climate, hygiene, diet, and exposure to vectors. • The mode of transmission varies with the type of worm; • ingestion of eggs or larvae, • penetration by larvae, • bite of vectors, • ingestion of stages in the meat of intermediate hosts. Worms are often long-lived.
Helminths • although infections are often asymptomatic, severe pathology can occur. • worms are large and often migrate through the body, they can damage the host's tissues directly by their activity or metabolism. • damage also occurs indirectly as a result of host defense mechanisms. • almost all organ systems can be affected.
Helminths are transmitted to humans in many different ways • by accidental ingestion of infective eggs (Ascaris, Echinococcus, Enterobius, Trichuris) • or larvae (some hookworms). • Other worms have larvae that actively penetrate the skin (hookworms, schistosomes, Strongyloides). • infection requires an intermediate host vector. • the intermediate vector transmits infective stages when it bites the host to take a blood meal (the arthropod vectors of filarial worms); • the larvae are contained in the tissues of the intermediate host and are taken in when a human eats that host (Clonorchis in fish, tapeworms in meat and fish, Trichinella in meat). • The levels of infection in humans therefore depend on • hygiene (as eggs and larvae are often passed in urine or feces), • climate (which may favor survival of infective stages), • the ways in which food is prepared, a • the degree of exposure to insect vectors.
Hookworms (Ancylostoma and Necator) actively suck blood from mucosal capillaries. • The anticoagulants secreted by the worms cause the wounds to bleed for prolonged periods, resulting in considerable blood loss. • Heavy infections in malnourished hosts are associated with anemia and protein loss. • Diversion of host nutrients by competition from worms is probably unimportant, but interference with normal digestion and absorption may well aggravate undernutrition. • The tapeworm Diphyllobothrium latum can cause vitamin B12 deficiency through direct absorption of this factor.
Many helminths undertake extensive migrations through body tissues, which both damage tissues directly and initiate hypersensitivity reactions. • The skin, lungs, liver, and intestines are the organs most affected. • Petechial hemorrhages, pneumonitis, eosinophilia, urticaria and pruritus, organomegaly, and granulomatous lesions • Feeding by worms upon host tissues is an important cause of pathology, particularly when it induces hyperplastic and metaplastic changes in epithelia. • liver fluke infections lead to hyperplasia of the bile duct epithelium. • Chronic inflammatory changes around parasites (for example, the granulomas around schistosome eggs in the bladder wall) have been linked with neoplasia
Immune-mediated inflammatory changes occur in the skin, lungs, liver, intestine, CNS, and eyes as worms migrate through these structures. • Systemic changes such as eosinophilia, edema, and joint pain reflect local allergic responses to parasites. • The pathologic consequences of immune-mediated inflammation are seen clearly in intestinal infections (especially Strongyloides and Trichinella infections). • Structural changes, such as villous atrophy, develop. • The permeability of the mucosa changes, fluid accumulates in the gut lumen, and intestinal transit time is reduced. • Prolonged changes of this type may lead to a protein-losing enteropathy. • The inflammatory changes that accompany the passage of schistosome eggs through the intestinal wall also cause severe intestinal pathology. • Heavy infections with the whipworm Trichuris in the large bowel can lead to inflammatory changes, resulting in blood loss and rectal prolapse.
Nemathodes (roundworms) • nematodes are cylindrical rather than flattened • the body wall is composed of • an outer cuticle that has a noncellular, chemically complex structure, • a thin hypodermis, • musculature. • The cuticle in some species has longitudinal ridges called alae. • The bursa, a flaplike extension of the cuticle on the posterior end of some species of male nematodes, is used to grasp the female during copulation.
Nematodes are usually bisexual. • Males are usually smaller than females, • a curved posterior end, and possess (in some species) copulatory structures, such as spicules (usually two), a bursa, or both. • The males have one or (in a few cases) two testes, which lie at the free end of a convoluted or recurved tube leading into a seminal vesicle and eventually into the cloaca.
Ascariasis • Ascaris lumbricoides • largest nematode (roundworm) parasitizing the human intestine • adult females: 20 to 35 cm; • adult male: 15 to 30 cm
Symptoms • High worm burdens may cause abdominal pain and intestinal obstruction. • Migrating adult worms may cause symptomatic occlusion of the biliary tract or oral expulsion. • During the lung phase of larval migration, pulmonary symptoms can occur • cough • dyspnea, • hemoptysis, • eosinophilic pneumonitis - Loeffler’s syndrome
Treatment • albendazole, • mebendazole, • pyrantel pamoate • The most effective method to control ascariasis, as well as other soil-transmitted helminthiasis, is sanitary disposal of feces. • Care must be taken in treating mixed helminthic infections involving A lumbricoides,because an ineffective ascaricide may stimulate the parasite to migrate to another location. Persons in whom asymptomatic ascariasis is detected incidentally should be treated to prevent the possibility of a future abnormal migration of these large worms into extraintestinal sites.
Drancunculus medinensis • Dracunculiasis (guinea worm disease) • isolated areas in a narrow belt of African countries
Humans become infected by drinking unfiltered water containing copepods (small crustaceans) which are infected with larvae of D. medinensis • Following ingestion, the copepods die and release the larvae, which penetrate the host stomach and intestinal wall and enter the abdominal cavity and retroperitoneal space. • After maturation into adults and copulation, the male worms die and the females (length: 70 to 120 cm) migrate in the subcutaneous tissues towards the skin surface. • approximately one year after infection, the female worm induces a blister on the skin, generally on the distal lower extremity, which ruptures. • when this lesion comes into contact with water, a contact that the patient seeks to relieve the local discomfort, the female worm emerges and releases larvae. • The larvae are ingested by a copepod and after two weeks (and two molts) have developed into infective larvae.
Symptoms • The worm emerges as a whitish filament (duration of emergence: 1 to 3 weeks) in the center of a painful ulcer, accompanied by inflammation and frequently by secondary bacterial infection.
Treatment • local cleansing of the lesion • local application of antibiotics because of bacterial superinfection. • mechanical, progressive extraction of the worm over a period of several days. • no curative antihelminthic treatment available • winding the protruding worm on a stick • because the worm protrudes only a few centimeters per exposure to water, this procedure takes, on average, three months to completely remove the worm.
Enterobius vermicularis • Enterobius vermicularis (previously Oxyuris vermicularis) • pinworm infection • adult females: 8 to 13 mm, • adult male: 2 to 5 mm • more frequent in school- or preschool- children and in crowded conditions
Eggs are deposited on perianal folds. • Self-infection occurs by transferring infective eggs to the mouth with hands that have scratched the perianal area. • Person-to-person transmission can also occur through handling of contaminated clothes or bed linens. • Enterobiasis may also be acquired through surfaces in the environment that are contaminated with pinworm eggs (e.g., curtains, carpeting). • Some small number of eggs may become airborne and inhaled. These would be swallowed and follow the same development as ingested eggs.
Symptoms • perianal pruritus, especially at night, • invasion of the female genital tract with vulvovaginitis , pelvic or peritoneal granulomas • anorexia, irritability, and abdominal pain. • The most common symptom is pruritus ani, which disturbs sleep and which, in children, may be responsible for loss of appetite. abdominal pain, irritability, and pallor • a cause of appendicitis, • female worms migrate up the vagina and fallopian tubes and into the peritoneal cavity, where they become encapsulated with granulomatous tissue. • Recurrent urinary tract infections have been attributed to ectopic pinworm infections.