Download
1 / 29
300 likes | 417 Views
Evaluation of Peripheral blood. Huang Jinwen Sir Run Run Shaw Hospital. Automated hematology instrumentation. WBC differential Advia 2120. Monocytes. Neutrophils.

E N D
Evaluation of Peripheral blood Huang Jinwen Sir Run Run Shaw Hospital
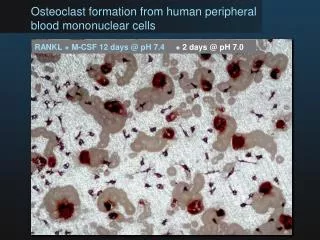
WBC differential Advia 2120 Monocytes Neutrophils Neutrophils (pink) and eosinophils (yellow) containing the most perox activity are found to the right. Cells with little or no perox cluster to the left, such as lymphocytes/basophils (blue) and large unstained cells (blasts, variant and atypical lymphocytes, light blue). Monocytes (green) contain a small amount of perox and are located between the neutrophils and large unstained cells. Noise is indicated in the lower left hand corner (white). blasts cell size Lymphocytes eosinophils peroxidase
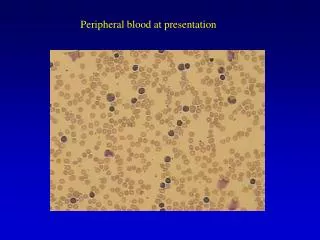
Red cell size distribution curves in hereditary sideroblastic anemia A broad population of red cells, varying markedly in size, with the majority of the cells being microcytic. Presence of two populations of red cells
Comparison between automated optical and immunologic platelet counts The majority of the data points well outside of the 95 percent confidence limits are above the best-fit line, suggesting that the optical method is more prone to overestimate platelet counts than the immunologic method in this range.
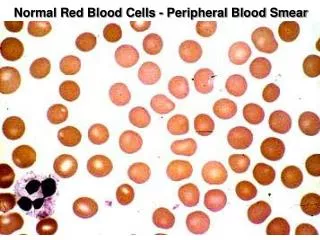
Optimal area for review Suboptimal blood smear Rouleaux in myeloma Normal peripheral blood smear
WBC Count • The normal limit in adults: 4.400 to 11.0. (4.0 to 10.0) x109/L • Leukocytosis: NL + 2SD, or> 11.0 x109/L • Hyperleukocytosis or leukemoid reaction: > 50.0 x109/L • Neutrophilic leukocytosis: >11.0 x109/L, + ANC>7,700 x109/L • ANC = WBC x percent (PMNs + bands) ÷ 100
Neutrophilic leukocytosis Infection, Stress, Smoking, Pregnancy, Following exercise. • It commonly seen in • It can also occur in • Neutrophilia Chronic myeloproliferative disorders, Chronic myeloid leukemia
Lymphocytic leukocytosis • WBC 11.0 X109/L, an absolute lymphocyte count > 4.8 X109/L . • Infectious mononucleosis and pertussis • Lymphoproliferative disorders, such as the acute and chronic lymphocytic leukemias
Monocytic leukocytosis • WBC> 11.0 x109/L, an absolute monocyte > 0.8 x109/L. • Acute and chronic monocytic variants of leukemia • Acute bacterial infection or tuberculosis • Monophilia.
Eosinophilic and basophilic leukocytosis • WBC>11.0 x109/L, an absolute eosinophil > 0.45 x109/L or basophil >0.2 x109/L • Eosinophilic leukocytosis can be seen in • Basophilic leukocytosis is a distinctly unusual condition, Chronic leukemia, Solid tumors, Infection with parasites, Allergic reactions, Following treatment with IL-2 Basophilic or Mast cell variants of acute or chronic leukemia
Regulation of neutrophil counts PMN development
Detection of infection or inflammation band count ≥20 cytoplasmic vacuoles left-shift Dohle bodies, Toxic granulation
The leukocyte alkaline phosphatase score • LAP is high in • LAP is low in Infection Inflammation Polycythemia vera Chronic myeloid leukemia Paroxysmal nocturnal hemoglobinuria
Definitions of neutropenia • Mild neutropenia: ANC 1.0 ~1.5 X109/L • Moderate neutropenia: ANC 0.500 ~1.0 X109/L • Severe neutropenia: ANC < 0.5 X109/L
Etiology of isolated neutropenia • Acquired neutropenias • Postinfectious neutropenia • Drug-induced neutropenia and agranulocytosis • Primary immune disorders • Hypersplenism • Bone marrow disorders • Congenital neutropenias • Myeloperoxidase deficiency
Risk Factors of Fever ■ A rapid decline in ANC or ANC <0.1 X109/L ■ Prolonged duration of neutropenia (>7 to 10 days) ■ Leukemic induction ■ Cancer not under control ■ Comorbid illnesses requiring hospitalization ■ Use of central venous catheters ■ Disruption of mucosal barriers ■ Use of monoclonal antibodies
INFECTIONS IN FEBRILE NEUTROPENIA ■A majority of patients had occult bacterial infections ■ An infectious source identified in ~ 30 % ■ Bacteremia documented ~25% ■ ~80% of identified infections arised from patients‘ own endogenous flora.
Laboratory studies • CBC with differential, transaminases, bilirubin, amylase and electrolytes, a chest radiograph, and cultures. • Two or more blood cultures, sputum Gram stain and culture, and urine Gram stain and culture. • Pulmonary infiltrates frequently can not produce sputum; a more invasive approach including bronchoscopy or open lung biopsy. • Lumbar puncture is not usually recommended.
Blood cultures • One set /day for a stable fever pattern. • Two or three sets initially and to wait 48 to 72 hours to repeat blood cultures.
Chest radiographs ■Findings are often minimal or absent even in patients with pneumonia. ■ Findings may develop along with an increase in symptoms as the neutropenia begins to resolve.
Chest CT scanning CT should be ordered for the patients with pulmonary symptoms.
Colony stimulating factors ■ CSF reported to decrease the duration of neutropenia, fever, and hospitalization. ■ CSF have not been shown to decrease mortality. ■ These agents should not be used routinely for patients with fever and neutropenia. ■ It may be appropriate to consider their use in critically ill patients.