Download
1 / 47
520 likes | 734 Views
KUWAIT UNIVERSITY FACULTY OF MEDICINE DEPARTMENT OF ANATOMY 210-Anatomy T. Chacko Mathew, M.Sc. Ph.D., FRCPath (UK). The Vertebral Column. OBJECTIVES:. At the end of the lecture the students should be able to describe

E N D
KUWAIT UNIVERSITYFACULTY OF MEDICINEDEPARTMENT OF ANATOMY210-Anatomy T. Chacko Mathew, M.Sc. Ph.D., FRCPath (UK)
OBJECTIVES: • At the end of the lecture the students should be able to describe • The structure and functions of the vertebral column (regions, number of vertebrae in each region) • The primary and secondary curves of the vertebral column • Structure of a typical vertebra • Structure of atypical vertebrae • Zygapophyseal joint, atlanto-occipital joint and atlanto-axial joint • Structure and function of the inter-vertebral disc • Common injuries and deformities of the vertebral column
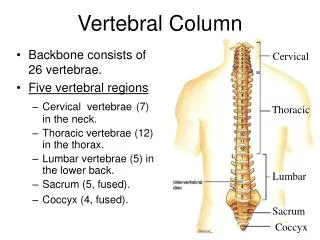
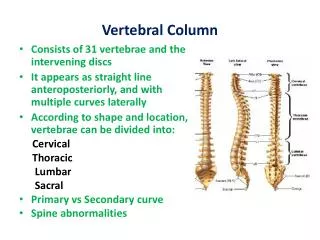
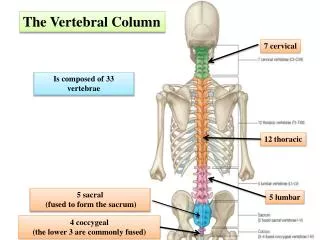
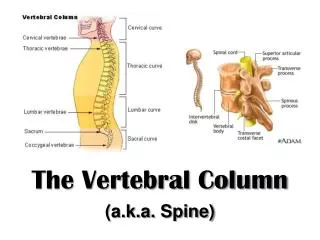
The vertebral column is composed of a series of 33 separate bones known as vertebrae. • There are seven cervical or neck vertebrae, • 12 thoracic vertebrae, • Five lumbar vertebrae. • The sacrum is composed of five fused vertebrae, • There are four coccygeal vertebrae (Lower three are commonly fused).
THE VERTEBRAL COLUMN FUNCTIONS: • Strong flexible rod providing movement of the trunk. • Encloses and protects the spinal cord and the spinal nerve roots. • It supports the head and acts as a pivot. • Serves as a point of attachment for ribs and acts as an axis of the body. • Plays an important role in maintaining the posture of the body and locomotion.
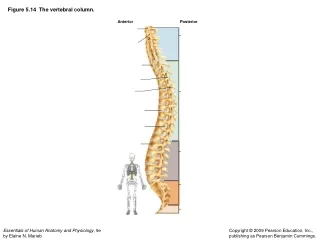
CURVATURES OF THE VERTEBRAL COLUMN • 2 primary (thoracic and sacro-coccygeal) • 2 secondary curvatures (cervical and lumbar). • These curves are called the cervical, thoracic, lumbar, and pelvic curves.
NORMAL CURVATURES OF THE VERTEBRAL COLUMN • In the early embryo, the vertebral column is C-shaped; pre-natal and post-natal growth accounts for 4 distinct curvilinear regions in the adult
Primary curvatures: posterior convexities • Present at birth; relatively immobile because of attachments to other skeletal components (rib cage and pelvis) • Thoracic • Sacral
Secondary curvatures: anterior convexities • Develop after birth; relatively flexible because of lack of other skeletal connections • These curves allow human beings to stand upright and help to maintain the balance of the upper body.
Secondary curvatures: anterior convexities • The cervical and lumbar curves are not present in an infant. • The cervical curves forms around the age of 3 months when an infant begins to hold its head up and the lumbar curve develops when a child begins to walk.
Kyphosis • Exaggerated posterior curvature, generally in the thoracic region (a "humpback")
Lordosis • Exaggerated anterior curvature, generally in the lumbar region (a "swayback")temporary lordosis is common among pregnant women
Scoliosis • Lateral curvature. • Most common abnormal curvature, occurring in 0.5% of the population; more common among females • may result from unequal growth of the two sides of one or more vertebrae
Each typical vertebra consists of an anterior body which joins with the vertebral arch posteriorly via short rounded bars, the pedicles.
The body is made of strong, thick, spongy bone which resists compression.
The arch bears 7 processes which mainly provide movement or muscular attachments. • These processes are: • a pair of transverse processes, • a pair of superiorarticular processes • a pair of inferior articular processes • a spinous process.
The superior and inferior articular processes bear superior and inferior articular facets to form synovial joints.
The spinous process is formed by the union of two flat leaf like oblong plates of bone with sloping surfaces, called the laminae. lamina lamina
The pedicles on their upper and lower surfaces form superior and inferior vertebral notches which ultimately contribute to the formation of intervertebral foramen containing the spinal nerve and its blood vessels.
Encircled by the body anteriorly, vertebral arch posteriorly and the pedicles laterally is the vertebral foramen, which lodges the spinal cord with its membranes and blood vessels. • The vertebral foramina of the successive vertebrae form the vertebral canal
The first cervical vertebra is known as the atlas. • It has no body. • It contains an anterior tubercle instead. • Its superior articular facets articulate with the occipital condyles of the skull. • The head thus moves forward and backwards on this vertebra.
The second cervical vertebra is known as Axis • It contains a prominent odontoid process, a tooth-like structure that projects superiorly from the body to articulate with the anterior arch of the atlas • It articulates with the anterior tubercle of the atlas, forming a pivotal joint. • Side to side movements of the head take place about this joint.
The seventh cervical vertebra is sometimes considered atypical since it lacks a bifid spinous process.
VERTEBRAL PROCESSES 7 IN NUMBER ON TYPICAL VERTEBRAE
Spinous Processes (1 per vertebra) • project posteriorly or posteroinferiorly in the median plane arise from the point of union of left and right laminae provide attachment for interspinous and supraspinous ligaments and several muscles
Transverse Processes (2 per vertebra: left and right) • Extend posterolaterally from the point of union of pedicles and laminae • Provide attachment for intertransverse ligaments and several muscles
Articular Processes (Zygapophyses) (4 per vertebra) • Left and right, superior and inferior • also arise from the junction of pedicles and laminae • Superior processes project superiorly and inferior processes project inferiorly (with characteristic regional variations).
Articular Processes (Zygapophyses) (4 per vertebra) • Each articular process bears a facet which articulates with a facet of an adjacent vertebrae to form a zygapophyseal (facet) joint
Zygapophyseal (facet) joints joints between articular processes of adjacent vertebral arches permit gliding movements between vertebrae
Atlanto-occipital joints • superior articular facets of the atlas are concave and kidney-shaped to receive the occipital condyles of the skull • facilitate nodding (flexion) of the head
Atlanto-axial joint • The dens of the axis (C2) articulates with the body of the atlas (C1) • Facilitates pivoting of the head
The bodies of adjacent vertebrae are connected by specialized cartilaginous joints known as intervertebral discs.
Each disc is composed of a central core of gelatinous material, known as the nucleus pulposus, and a surrounding series of fibrous rings known as the annulus fibrosis Normally body weight is transmitted through the disc by loading the nucleus pulposus, which is then compressed and transfers its loading to the annulus fibrous.
In most individuals, the fibers of the annulus fibrosus effectively resist this load, but in some people they do not and the nucleus pulposus is forced out of the disc, or is herniated. A herniated nucleus pulposus can have a profound effect on the adjacent spinal nerves
Two ligaments connect the vertebral bodies anteriorly and posteriorly and thereby reinforce the intervertebral disc. 1. The anterior longitudinal ligament is strong and robust throughout
But the posterior longitudinal ligament becomes thin and narrow in the lumbar region. This change in structure of the posterior longitudinal ligament is part of the reason that the overwhelming majority of disc herniations occur posteriorly in the lumbar region.
SPONDYLYSIS; SPONDYLOSIS Chronic degenerative disease of intervertebral discs and/or vertebral bodies. May compress spinal cord, nerves, or roots. If symptoms present, most often present as radiculopathies
SPINAL CORD TRANSECTION Results in loss of all sensation and voluntary movement inferior to the lesion • Paraplegia: Paralysis of lower body including both lower extremitiesResults from spinal cord transection between cervical and lumbosacral enlargements • Quadriplegia: Paralysis of all four limbs. Results from spinal cord transection superior to C3
SCIATICA • Pain resulting from irritation of the sciatic nerve • Usually caused by compression or trauma to the sciatic nerve or its roots
RADICULOPATHIES • Shooting pain that radiates down one or both legs in a dermatomal distribution, often with associated sensory and motor impairment • Usually caused by compression or stretching of spinal nerves or roots
OSTEOPOROSIS • Most common in postmenopausal women • Loss of endogenous estrogen leads to severe decrease in vertebral bone density, due to demineralization • Characterized by dorsal kyphosis - Commonly presents medically as a vertebral compression fracture. Can be prevented or slowed by hormone replacement therapy.