Download
1 / 49
690 likes | 1.66k Views
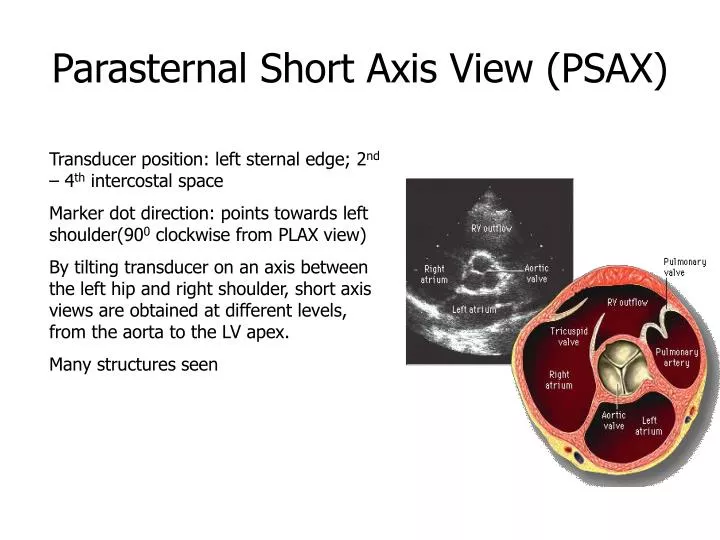
Parasternal Short Axis View (PSAX). Transducer position: left sternal edge; 2 nd – 4 th intercostal space Marker dot direction: points towards left shoulder(90 0 clockwise from PLAX view)

E N D
Parasternal Short Axis View (PSAX) Transducer position: left sternal edge; 2nd – 4th intercostal space Marker dot direction: points towards left shoulder(900 clockwise from PLAX view) By tilting transducer on an axis between the left hip and right shoulder, short axis views are obtained at different levels, from the aorta to the LV apex. Many structures seen
Papillary Muscle (PM)level PSAX at the level of the papillary muscles showing how the respective LV segments are identified, usually for the purposes of describing abnormal LV wall motion LV wall thickness can also be assessed
Apical 4-Chamber View (AP4CH) Transducer position: apex of heart Marker dot direction: points towards left shoulder The AP5CH view is obtained from this view by slight anterior angulation of the transducer towards the chest wall. The LVOT can then be visualised
Apical 2-Chamber View (AP2CH) Transducer position: apex of the heart Marker dot direction: points towards left side of neck (450 anticlockwise from AP4CH view) Good for assessment of LV anterior wall LV inferior wall
Sub–Costal 4 Chamber View(SC4CH) Transducer position: under the xiphisternum Marker dot position: points towards left shoulder The subject lies supine with head slightly low (no pillow). With feet on the bed, the knees are slightly elevated Better images are obtained with the abdomen relaxed and during inspiration Interatrial septum, pericardial effusion, desc abdominal aorta
Hemodynamic states • Normal • Hypovolemia • Vasodilatation • Systolic failure • Diastolic failure • Systolic and diastolic failure • RV failure
Case discussion? • 75yr male for hip surgery • Starting BP 140/90 down to 85/50 after 10 mins of anesthesia • HR unaltered lil bit improvement with aramine fall back to 80/50 • CVL inserted RA pressures 17 mm hg • PA Catheter: CI 1.8l/min/m2 & PCWP of 18 • What next????????? • TTE
Hemodynamic assessment • Estimate volume • Estimate systolic function • Estimate filling pressures • Final assessment (Put all together)
Estimate LV end diastolic vol ( preload) M mode; Simpsons biplane etc • Estimate LV systolic function Eye balling; FS; FAC; EF • RV systolic function mostly qualitative • Estimate LA pressures: Intra atrial septum; LA size; surrogate from RA pressures • Estimate RA pressures : IVC
Final Assessment • Normal : LVEDA; EF & LAP normal • Hypovolemia : LVEDA & LAP ; EF = or • Diastolic failure : LVEDA ; LAP ; EF = • Systolic failure : LVEDA ; LAP =; EF • Systolic & diastolic: LVEDA & LAP ; EF • RV failure : RV vol; LAP • Vasodilatation : LVEDA & LAP =; EF
Normal Echo Dimensions • LV Diastolic Dimension: 3.7-5.5 cm • LV Systolic Dimension: 2.0-4.0 cm • Interventricular septum* (Diastole): 0.6-1.1cm • LV Posterior Wall* (Diastole): 0.6-1.1cm • LVOT diameter (Systole): 1.8-2.2 cm • Aortic Root** (Diastole): 2.0-3.7 cm • Left Atrium (Systole): 2.0-4.0 cm • Left Atrial Area (4 chamber): <20cm2 • Left Atrial Volume/m2 BSA: 16-28 ml • RV Diastolic Dimension: 0.9-2.5 cm