Download
1 / 5
50 likes | 143 Views
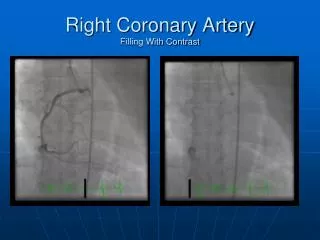
Pulmonary edema (yellow arrow) in a 12-yr-old patient with mitral regurgitation post mitral valve replacement (red arrow) complicated with fungal endocarditis (blue arrow). RCA. LCA. AO. On short-axis view, left and right coronary artery aneurysms were

E N D
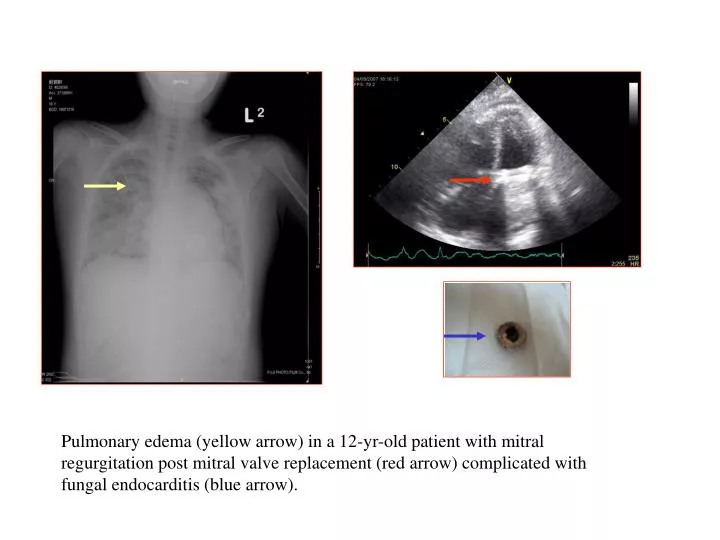
Pulmonary edema (yellow arrow) in a 12-yr-old patient with mitral regurgitation post mitral valve replacement (red arrow) complicated with fungal endocarditis (blue arrow).
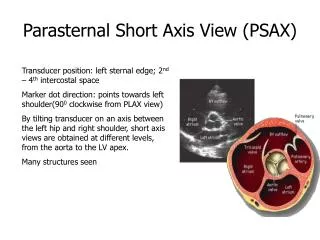
RCA LCA AO On short-axis view, left and right coronary artery aneurysms were shown in a 5-year-old boy with Kawasaki disease complicated with coronary aneurysm. M-mode showed poor LV wall motion.
RV LV RA On parasternal short-axis view, the presence of a color flow jet from LV to RV (white arrow) was shown in a 6-month-old female infant with mb-VSD.
RAO view LAO view Ablation (arrow) of idiopathic left ventricular tachycardia in the basal septal area of LV in a 15-yr-old boy.
Procedures for transcatheter implantation of the ADO device in PDA. (A) Lateral projection of the aortogram showing the PDA with a diameter of 3.5 mm and Qp/Qs >3 and elevated pulmonary arterial pressure in a neonate. (B) Kinking of the sheath in the pulmonary artery during the advancing of the delivery cable and device. (C) The kinking was obliterated by slowly withdrawing the sheath while advancing the device until the retention skirt was deployed in the descending aorta. The whole delivery system was pulled firmly until the retention skirt was optimally fit in the ampullae. (D) The body of the device was deployed by gently withdrawing the sheath. (E) Position and conformation of the device was verified by angiogram. (F) The device was relieved.