Download

1 / 12
180 likes | 893 Views
Training on entering data in patient tab in Argus safety database. Global pharmacovigilance department. Patient information screen. If reporter is also the reporter, clicking this button will autopopulate the patient information from the reporter data.

E N D
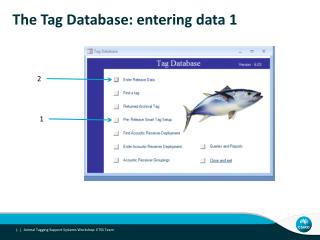
Training on entering data in patient tab in Argus safety database Global pharmacovigilance department
Patient information screen If reporter is also the reporter, clicking this button will autopopulate the patient information from the reporter data Only to be used for children cases associated to maternal pregnancy cases or 'Drug Exposure via the Father' cases Captures history and current status of the patient. These fields map to German BfArM tab in the analysis tab Do not check Name of the patient Check only if it is a child case for a parent/child case Address of the patient Occupation of the patient Ethnicity of the patient Date of birth of the patient Gender of the patient Autopopulated field Height of the patient LMP date, only for pregnancy cases Age of the patient. If the patient age is more than 120 years, do not enter the age in the structured field. Mention the age in the case narrative. Select “Yes” if the patient is pregnant. For male patients this field is greyed out. If selected “Pregnancy Information” screen is enabled. Weight of the patient. If weight of the patient is more than 650 kg, do not enter in the structured field. Include this information in the case narrative
Pregnancy information screen Initial reports of pregnancy received where the outcome of the pregnancy has already occurred. Initial reports of pregnancy where no outcome is known at the time the initial report is received No. of weeks of pregnancy at the time of exposure Pregnancy due date Trimester(s) during which the patient was exposed to the drug Weight of the baby Apgar score of the neonate The date of delivery Type of delivery Type of birth Any delivery notes Pregnancy outcome Click to add information about multiple neonates
Parent information Include the information of the parent who was the source of transmission of the drug. If the source is the father, the information regarding the father would be added in the parent information section. Enabled only for the female patients Medical history of the parent If both the parents are a source of drug, then the mother’s information should be added in the parent information section. The father’s information should be added in the case narrative.
Other Relevant History To move up or down the history conditions To delete the history To add one more history field To encode through the dictionaries To copy the condition Start date and end date Coded terms are displayed Enter additional notes if required If condition is ongoing Select the condition through the codelist
Entering past drugs To move up or down the past drugs Enter the name of the drug. It will be coded through WHO drug dictionary. Click “Encode” button and select drug from the pop up 'Drug Coding - WHO Web Page Dialog' box To add more past drugs, click “Add” button. If coded through WHO DD the red cross sign changes to green tick Select “historical drug” from the codelist. To copy past drug Start and stop date of taking the drug in the past Displays the coded drug Displays the MedDRA code Enter any additional comments Displays the MedDRA code Indication for which the drug was used. Adverse reaction, if any experienced by the patient in the past with the use of this drug. Check if the drug is still being continued. Checking this field will grey out the drug stop date field. All drugs that were completed/discontinued before the start of the treatment with the suspect drugs should be coded as historical drug.
Entering past disease To delete a past disease To copy a past disease Adverse event term as reported If coded through MedDRA, red cross changes to green tick Select “historical AR” from the codelist. Selecting this option, enables only the “Verbatim” field. To add history condition Start and stop date Any clarification notes, if required. Check if the past disease is still ongoing. Checking this field will grey out the stop date field.
Entering lab data Select if test result is normal, depressed, normal or elevated from the codelist. If same test was repeated, add more dates To add more tests Unit of the test result Date when the test was done Test result Click to code through MedDRA Test name as reported Test code selected from MedDRA. Select unit of the test from the codelist Enter “See relevant text field” in this field to enter the test results for investigations which do not have numerical values e.g. ECG and biopsy results. Enter the data in the relevant test field. Add normal low value, if known Add normal high value, if known
All tests relevant to the ADR should be captured in the field for lab tests. • If you cannot code a particular laboratory test, enter it in the free text field specifying the test name, date it was performed and the results. See example: 01 Feb 2013 (Neurological examination) – Found possible stroke and signs of neurodegenerative disease.
Event Death Details section • Data is already entered at the time of book in. Check if the data entered is correct.