Download
1 / 23
• 230 likes • 433 Views
Subclinical Neck Pain and the Effects of Cervical Manipulation on Elbow Joint Position Sense. Heidi Haavik, PhD, BSc (Chiro), and Bernadette Murphy , PhD, DC J Manipulative Physiol Ther 2011:34:88-97. Background. Segmental restriction may lead to maladaptive neuroplastic changes.

E N D
Subclinical Neck Pain and the Effects of Cervical Manipulation on Elbow Joint Position Sense Heidi Haavik, PhD, BSc (Chiro), and Bernadette Murphy, PhD, DC J Manipulative PhysiolTher 2011:34:88-97
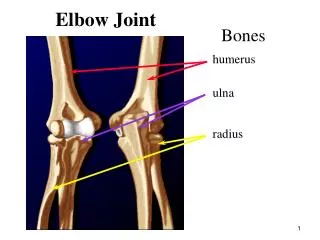
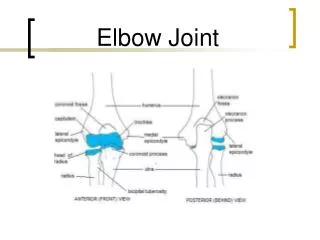
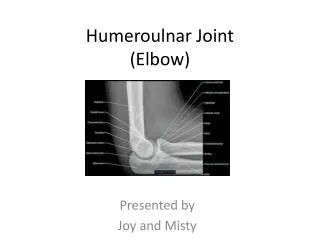
Background • Segmental restriction may lead to maladaptive neuroplastic changes. • These changes have been implicated in long-term pain conditions and may cause changes in proprioception. • Cervical spinal dysfunction disturbs proprioception from the neck and upper limb. • Head and neck position may also influence upper limb proprioception. • Reduced accuracy of elbow joint position sense (JPS). • Subclinical Neck Pain (SCNP) • Definition: Reoccurring neck dysfunction such a mild neck pain, ache, and/or stiffness with or without a history of known neck trauma. Do not have constant symptoms and have not sought treatment. • Use: Explore neurophysiologic dysfunction without the confounding effect of pain.
Hypotheses • Restricted segments of the spine may represent an ongoing state of altered afferent input that could induce maladaptive neuroplastic changes possibly impacting proprioception. • High-velocity, low-amplitude (HVLA) manipulation has a neuromodulatory effect on central nervous system (CNS) function, thus spinal manipulation may improve central proprioceptive processing.
Aims • Determine whether elbow JPS accuracy differs between subclinical neck pain (SCNP) participants and those with no history of any neck symptoms or injury • Determine whether manipulating (adjusting) dysfunctional cervical segments in the SCNP group can improve the accuracy of the elbow JPS.
Experimental Protocol • 2 groups: SCNP (n=25) (no acute pain but history of subclinical pain) vs. Healthy control (n=18) (no history of neck pain or injury). • Control: 11/18 had no intervention to assess for learning and boredom effects. • Exclusion: History of shoulder/elbow pain, current pain anywhere in the body, diagnosis of degenerative joint disease (DJD), anything effecting the sensory system, and if they sought treatment. • 14/25=had a previous head, neck, whiplash injury.
Experimental Protocol Also assessed for cervical dysfunction Continuous EMG ensured total rest throughout passive and rest conditions of the data collection procedure.
Experimental Protocol 4 things that reduced sensory cues: Cloth doughnut (elevated arm so forearm did not touch the surface. Eyes were closed during each experimental condition. JPS was performed at the midrange movement to decrease cues from skin/tendon stretch and joint contact at end ROM. Speed of arm positioning varied.
Data and Statistical Analysis Accuracy (i.e. angle reproduction) was assessed using 3 parameters: • Absolute Error-magnitude of the error; absolute difference (in either direction). • Constant error-direction and magnitude of error (diff. b/w the presented and reproduced angles). • Variable error-standard deviation (SD) of the mean constant error.
Data and Statistical Analysis • Overall accuracy • Multifactorial ANOVA • GROUP (SCNP vs. control group) • CONDITION (neutral, flexion, left rotation, and combined flexion with left-rotation) • Effect of adjusting dysfunctional segments • Multifactorial, repeated measures ANOVA • TIME (pre and post measures) • CONDITION (neutral, flexion, left rotation, and combined flexion with left-rotation) • GROUP (SCNP vs. control group) • Pairwise comparisons of pre/post intervention data.
Results Absolute Error: Overall group effect comparing pre-intervention data. Control group significantly better (p=.04). • FYI… • Absolute Error-magnitude of the error; absolute difference (in either direction). • Constant error-direction and magnitude of error (diff. b/w the presented and reproduced angles). • Variable error-SD of the mean constant error.
Results • The effect of cervical adjustments: • Significant interactive effect for TIME , GROUP, and HEAD POSITION (p=.008). • Significant interactive effect for TIME and GROUP (p<.001). • Further analysis of SCNP • Overall effect for TIME (p<.001) • Significant interactive effect for TIME and HEAD position (p=.025).
Results • A priori pairwise comparisons of pre/post adjustment data. • Significant improvement in JPS after adjustments when the participants had their heads in: • Neutral (p<.04) • Full left rotation (p=.01)
Results • When participants were asked to repeat previously presented angle: Neutral control position • Before neck manipulation • Mean absolute error 3.31 (95% CI 2.93-3.68) • After neck manipulation • Mean absolute error decreased • 2.47 (95% CI 2.11-2.83) Full left rotation • Before neck manipulation • Mean absolute error=3.69 (95% CI 3.13-4.25). • After manipulation • Mean absolute error=2.90 (95% CI 2.49-3.31).
Results • Control group data: • Significant overall effect with the control participants less able to accurately repositioning their arms after the control intervention (p=.03). *?
Results • No significant group differences in variance (fig.3?). • Variance data assessing any effect from cervical manipulation revealed a significant interactive effect (p=.03), with variance error decreasing significantly after the adjustment. • Analysis of control group, significant overall effect (p<.001), with variance increasing significantly after the control.
Results • No significant group differences in constant error (fig.3?). • The interventions had no significant effect on constant error. • No significant effect due to head position was found in any of the calculated variables for either group, neither before nor after either intervention. • No significant group differences in background EMG for any muscle nor were there any changes in background EMG for any muscle after either intervention.
Conclusion by Authors • Participants with a self-reported history of SCNP have significantly worse elbow JPS compared to people that have no neck complaints and that a single session of HVLA adjustments of dysfunctional cervical joints resulted in a significant improvement of elbow JPS.
Discussion • Head and neck positions did not worsen JPS. • Possible methodological differences between this and previous studies. • In neck pain patients, proprioception and motor control rather than pain may be the “main factors” in the clinical picture. • This study: SCNP had worse JPS accuracy than control supports this. • Deficits in proprioception may be partly due to segmental dysfunction, which chiropractors treat. • Manipulation improved JPS accuracy in SCNP • Beneficial neuromodulaty effect • Dysfunctional segments, which may a source of altered afferent signaling leading to altered sensorimotor integration, may be normalized by HVLA-SM.
Limitations/Bias • Control- JPS accuracy was worse after control intervention. • Possible reasons why this occurred: • Time between pre/post measures (arms falling asleep) • Use of the supine position may have lead to upper limb sensory disturbances (vs. a reliable seated patient position). • Boredom effect in control • Placebo effect in SCNP • Avis Effect (participants responded because they were involved in a study).
Journal Club Discussion • What were the weaknesses of the article? • What were the strengths? • Are you convinced that SCNP participants have worse elbow JPS? • Do you feel that cervical spinal manipulation improved elbow JPS?
Thank You! • Thank you for attention! • Thank you Dr. Reed!