Download

1 / 57
570 likes | 867 Views
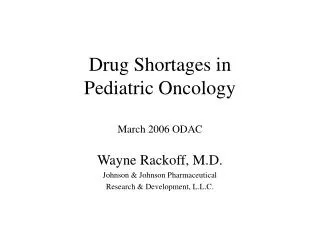
PEDIATRIC ONCOLOGY . CANCER; 10%. congenital anomalies; 8%. accidents; 44%. h e art disease; 4%. meningitis; 1%. other; 22%. Leading causes of death of children between of 1 and 14. HIV infection; 1% Homicide, 1%. Suicide, 1%. Pneumonia, 2%. cerebral palsy; 1%.

E N D
CANCER; 10% congenital anomalies; 8% accidents; 44% heart disease; 4% meningitis; 1% other; 22% Leading causes of death of children between of 1 and 14 HIV infection; 1% Homicide, 1% Suicide, 1% Pneumonia, 2% cerebral palsy; 1%
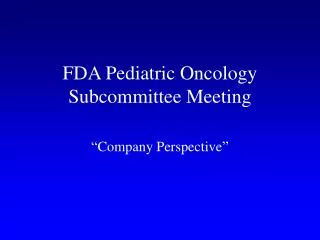
Distribution of cancer in children younger than 15 years of age by diagnosis
Etiology and mechanisms of carcinogenesis. • Endogenous factors: constitutional chromosomal abnormality; mendelian autosomal dominant, recessive, or X-linked patterns; non-mendelian inheritance; mutations in multiple genes or mitochondrial DNA or caused by mutations affecting imprinted genes.
Etiology and mechanisms of carcinogenesis. Exogenous factors: - physical agents most commonly studied are ultraviolet radiation, ionizing radiation, and extremely low-frequency (50-60 Hz) magnetic fields. - chemical factors are environmental pollutants, tobacco, aflatoxin, and androgenic steroids. - biologic agents.
Prenatal diagnosis of tumors (sonographic features) • Absence or disruption of contour, shape, location, sonographic texture or size, of a normal anatomic structure; • Presence of an abnormal structure or abnormal biometry; • Abnormality in fetal movement; • Polyhydramnios; • Hydrops fetalis.
Common chief complaints given by parents that suggest a pediatric cancer
Noninvasive imaging techniques • Plain film chest radiography • Plain films of the abdomen • Barium studies • Diagnosticultrasound (US) examination • Computed tomography (CT) • Magnetic resonance imaging (MRI) • Tumor markers • Excisional and incisional biopsies
TERATOMAS • Teratomas are tumors comprising more than a single cell type derived from more than one germ layer. A significant degree of confusion has arisen regarding nomenclature for the various subtypes of teratomas. The word itself is derived from the Greek word teraton, meaning monster, and was used initially by Virchow in the first edition of his book on tumors, which was published in 1863. Teratomas range from benign, well-differentiated (mature) cystic lesions to those that are solid and malignant (immature). Besides being mature, with malignant transformation, teratomas also may be monodermal and highly specialized.
The most common location • sacrococcygeal (57%) • gonads (29%) • mediastinal (7%) • retroperitoneal (4%) • cervical (3%) • intracranial (3%)
Classification of the sacrococcygeal teratomas • Type I tumors are predominantly external, attached to the coccyx, and may have a small presacral component (45.8%). No metastases were associated with this group. • Type II tumors have both an external mass and significant presacral pelvic extension (34%) and have a 6% metastases rate. • Type III tumors are visible externally, but the predominant mass is pelvic and intraabdominal (8.6%). A 20% rate of metastases was found in this group. • Type IV lesions are not visible externally but are entirely presacral (9.6%) and have an 8% metastases rate.
Malignant sacrococcygeal teratoma Sacrococcygeal teratoma <> <> Complications
Complicationsof the sacrococcygeal teratomas • associated congenital anomalies • pre-term labor and delivery • massive hemorrhage into the tumor with secondary fetal exsanguination • dystocia, secondary to tumor bulk or tumor rupture • placentomegaly and/or hydrops evolved, which, in turn, precipitated rapid fetal death
Differential diagnosis: • мeningomyelocele • rectal abscess • dermoid cyst • angioma • lipoma • neurogenic tumor • pilonidal cyst.
Treatment • Surgical, including removal of the coccyx. • Malignant = surgical excision + chemotherapy + radiation (metastases to lung, bone, liver).
Prognosis of the sacrococcygeal teratomas • Benign - disease free survival is greater than 90%; malignant - significant mortality, although good progress has been made recently in treatment of these tumors. Time of diagnoses is key: • < 2 months of age, only 7-10% are malignant • Age 1 year, 37% malignant • Age 2 years, 50% malignant
RHABDOMYOSARCOMA A malignant tumor of mesenchimal cell origin is called a sarcoma. Mesenchymal cells normaly mature into skeletal muscle, smooth muscle, fat, fibrous tissue, bone, and cartilage. Rhabdomyosarcoma is thought to arise from immature mesenchimal cells that are committed to skeletal muscle lineage, but these tumors can arise in tissues in which striated muscle is not normally found, such as urinary bladder. Rhabdomyosarcoma (RMS), the most common soft tissue sarcoma in infants and children, represents about 5-15% of all malignant solid lesions. RMS arises from a primitive cell type and occurs in mesenchymal tissue at almost any body site excluding brain and bone.
The Intergroup Rhabdomyosarcoma Study divides tumors into 5 types: • embryonal (57 %), • alveolar (19 %), • botryoid (6 %), • undifferentiated (17 %), • pleomorphic (1 %).
Alveolar rhabdomyosarcoma <> <>
Diagnosis. Biopsy (open, percutaneous, or endoscopic) is required for diagnosis and histological typing, which directs therapy. The extent of the tumour is defined by imaging techniques such as ultrasound, computed tomography (CT), or magnetic resonance imaging (MRI).
Treatment is determined on an individual basis, according to the site, stage, and histological type of the tumor. Treatment of rhabdomyosarcoma should be multimodal, consisting of chemotherapy, surgery, and radiotherapy.
Surgery is the most rapid way to ablate the disease, and it should always be used if subsequent function or cosmetic will not be greatly impaired. In sites such as vagina and urinary bladder and most head and neck sites, incisional biopsy (for diagnosis) may be the only feasible surgical procedure because of proximity to vital blood vessels and nerves, cosmetic consideration, or both. The second-look operation is used to resect residual tumor after the administration chemotherapy or local radiotherapy.
Radiation therapy can eradicate residual tumor cells from sites where surgical therapy alone cannot ablate the mass, especially in the head, neck, and pelvis.
Preoperative chemotherapy may reduce the extent of surgery required and should be considered. Postoperative chemotherapy is helpful in eradicating residual disease and micrometastases. Chemotherapy is the primary treatment for patients with metastatic disease at presentation. The commonly used drugs are a combination of cyclophosphamide, vincristine, actinomycin D, and Adriamycin. Doxorubicin, DTIC (ditriazoimidazole carboximide), cisplatin, and ifosfamide have also been known to be effective agents.
Wilms’ tumor is thought to be caused by alterations of genes responsible for normal genitourinary development. Examples of common congenital anomalies associated with Wilms’ tumor are cryptorchidism, double collecting system, horseshoe kidney, and hypospadias. Environmental exposures, although considered, seem less likely to play a role.
Clinical History.The most common presentation is an asymptomatic abdominal mass discovered by the parent or physician. Occasionally the child presents with haematuria, but symptoms are often non-specific: abdominal fullness, abdominal pain, gastrointestinal upset, fever, weight loss, malaise, and anaemia. Hypertension is sometimes detectable. A small number of patients who have hemorrhaged into their tumor may present with signs of hypotension, anemia, and fever. Rarely, patients with advanced-stage disease may present with respiratory symptoms related to the presence of lung metastases.
Cytogenetics studies • An 11p13 deletion as in the WAGR syndrome (Wilms’, aniridia, genitourinary abnormalities, mental retardation) • A duplication of the paternal allele 11p15 as in BWS • Mutational analysis of the WT1 gene in cases where Denys-Drash syndrome (intersexual disorders, nephropathy, Wilms’ tumor) is suspected
Imaging Studies • Renal ultrasonography(with dynamic imaging of the renal vein and interior vena cava). • CT scanning. Abdominal CT scanning helps determine the tumor's origin, lymph node involvement, bilateral kidney involvement, and invasion into major vessels (eg, inferior vena cava or liver metastases). If findings on chest CT scanning are positive while chest radiographic findings are negative, diagnostic biopsy of the lesions noted on the chest CT scan is recommended. • Chest radiography (4-field) - Detects lung metastases (Patients with lung lesions on chest radiography receive whole lung radiotherapy.)
<> nephroblastoma: angiograma
Complications. • The primary treatment, nephrectomy, may damage kidney function. However, additional treatment modalities may cause damage to several organs such as the heart, lungs, liver, bones, and gonads. In addition, both chemotherapeutic agents and radiation therapy can induce second malignant neoplasms.
NEUROBLASTOMA Neuroblastoma is a tumour of neural crest origin which may occur in the adrenal medulla or anywhere along the sympathetic ganglion chain, namely in the neck, thorax, abdomen, and pelvis. Seventy-five per cent of tumours occur in the abdomen (adrenal medulla 50 %, paraspinal ganglia 25 %), 20 % occur in the thorax, and 5 % occur in the neck and the pelvis.
Localizations of the neuroblastoma • 75 % of tumours occur in the abdomen: • adrenal medulla 50 %, • paraspinal ganglia 25 % • 20 % occur in the thorax, • 5 % occur in the neck and the pelvis
The Evans classification for neuroblastoma • Stage I: tumor confined to an organ of origin. • Stage II: tumor extending beyond an organ of origin, but not crossing the midline. Ipsilateral lymph nodes may be involved. • Stage III: tumor extending beyond midline. Bilateral lymph nodes may be involved. • Stage IV: remote disease involving skeleton, bone marrow, soft tissue or distant lymph nodes. • Stage IVS: same as stage I or II with presence of disease in liver, skin or bone marrow.
Diagnosis Ultrasonography distinguishes neuroblastoma (solid, extrarenal) from cystic lesions and renal tumours. The radiographic detection of calcification in the tumour is suggestive of neuroblastoma. In children with an abdominal neuroblastoma, intravenous urography shows displacement rather than distortion of the pelvicaliceal system. A skeletal survey and chest radiograph are mandatory to detect possible metastases. CT gives good anatomical data about the tumour. Recent studies suggest that magnetic resonance imaging (MRI) is useful both to delineate the primary tumor and to evaluate bone marrow metastasis, vessel involvement, and extension into spinal cord.
Treatment. The treatment modalities traditionally employed in the management of neuroblastoma are surgery, chemotherapy, and radiation therapy. The role of each method is determined by the natural history of individual cases considering stage, age, and histological features.
Surgery plays the pivotal role in the management of neuroblastoma. Depending of the timing, operative procedures can have diagnostic as well as therapeutic functions. The goals of primary surgical procedures, performed before any other therapy, are to establish the diagnosis, to provide tissue for biological studies, to stage the tumor surgically, and to attempt to excise the tumor, if feasible. In delayed primary or second look surgery, the surgeon determines response to therapy and removes residual disease when possible.
Chemotherapy is the predominant modality of management in management in neuroblastoma. Cyclophosphamide, vincristine, cisplatin, and doxorubicinare are the cornerstone of multiagent management. Drug combinations have been developed that take advantage of drug synergism, mechanism of cytotoxicity, and differences in side effects.
Radiation therapy has been used in the multimodality management of residual neuroblastoma, bulky unresectable tumors, and disseminated disease. More recently, the role of radiation therapy in neuroblastoma continues to be refined with the improviment in multiagentchemotherapyand the increasing trend toward developing risk-related treatment groups based on age, stage, and biologic features.
Vascular malformations (flat lesions) Salmon patch (also known as nevus simplex or nevus telangiectaticus) Port-wine stain (also known as nevus flammeus) Hemangiomas (raised lesions) Superficial hemangioma (Cherry, strawberryhemangioma) Deep hemangioma (also known as cavernous hemangioma) Classification of Vascular Lesions
After treatment Before treatment