Download
1 / 69
690 likes | 775 Views
Explore the immunopathogenesis, pathophysiology, and impact of bee sting envenomation on the human body, including anaphylaxis reactions and evolutionary insights. Discover the science behind anaphylactic shock, immune responses, and host factors influencing severity.

E N D
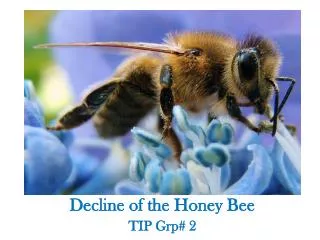
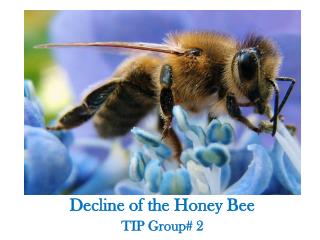
The pathophysiology of Honey Bee sting envenomation- and the effect on the body Dr Lynne Hepplestone BVSc
Abstract: Anaphylaxis is a severe systemic hypersensitivity reaction that is rapid in onset; characterized by life-threatening airway,breathing, and/or circulatory problems; and usually associated with skin and mucosal changes. Because it can be triggered in some persons by minute amounts of antigen (eg, certain foods or single insect stings), anaphylaxis can be considered the most aberrant example of an imbalance between the cost and benefit of an immune response. This review will describe current understanding of the immunopathogenesis and pathophysiology of anaphylaxis, focusing on the roles of IgE and IgG antibodies,immune effector cells, and mediators thought to contribute to examples of the disorder. Evidence from studies of anaphylaxis in human subjects will be discussed, as well as insights gained from analyses of animal models, including mice genetically deficient in the antibodies, antibody receptors, effector cells, or mediators implicated in anaphylaxis and mice that have been ‘‘humanized’’ for some of these elements. We also review possible host factors that might influence the occurrence or severity of anaphylaxis. Finally, we will speculate about anaphylaxis from an evolutionary perspective and argue that, in the context of severe envenomation by arthropods or reptiles, anaphylaxis might even provide a survival advantage. (Journal Allergy Clin Immunol 2017;140:335-48.) The pathophysiology of anaphylaxisLaurent L. Reber, PhD, Joseph D. Hernandez, MD, PhD, and Stephen J. Galli, MDc (Paris, France, and Stanford,California).
Case Report Bee Sting EnvenomationSudhansu Sekhar Sethi, Manoj Kumar Jena Abstract: Among the invertebrates, insects, particularly hymenoptera, most commonly cause anaphylaxis. In stinging bees, wasps and ants, the ovipositor of female has been modified into a stinger. Honey bees leave behind their barbed stinger in the victim’s body and eventually die by evisceration. Bee sting in most of the situations is potentially serious, the severity and duration of reaction varies from one person to another depending on location and number of bee stings received. The spectrum of bee sting disease ranges from local reaction to death. Stings from bees usually cause a transient local reaction which may last for several days and generally resolves without treatment. Occasionally death may occur mostly due to anaphylactic shock. Non anaphylactic causes of death are mainly due to multi organ failure. Honey bee sting is responsible for large number of casualty in tropical and subtropical countries • (J Indian Acad Forensic Med. April-June 2015, Vol. 37, No. 2)
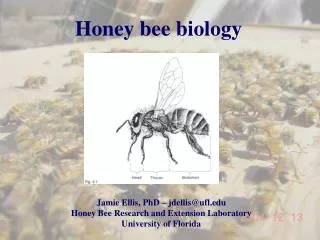
Scientific classification of the East African lowland Honey Bee(Linnaeus) • Kingdom Animalia • Phylum Arthropoda • Class Insecta • Family Apidae • Order Hymenoptra • Genus Apis • Species A.mellifera • Subspecies A.mellifera scutellata, A.mellifera capensis • RSA has Only One specie of Honey Bee (A. mellifera) which has 2 subspecies • They have ** the same venom ** • The variations in risks when stung lie with the host-that’s-stung, not with the bee nor its’ venom
Our African Honey Bee? • The East African lowland honey bee sting is no more venomous than a single European bee sting, • though East African lowland honey bees respond more quickly when disturbed than do European honey bees. • They send out three to four times as many workers in response to a threat. • They will also pursue an intruder for a greater distance from the hive.
All the components • Bee sting – the antigen (venom) • (antigenic stimulation) • Antibodies (IgE) • Effector cells (Mast cells, Basophils, Platelets) • Mediators (Histamines H1, H2) • (Inflammatory mediators)
Type 1 hypersensitivity reaction(Gell and Coombs system) • Antigen-bound IgE • Attaches to a (Fc) receptor on a Mast cell • The mast cell degranulates • Downstream signaling of cellular responses • Cascade of physiological changes • = reaction to a bee sting
Type 1 hypersensitivity reactions(Gell and Coombs) • Examples: • Honey bee stings • Venomous Snake bite • Vaccine reactions • Food sensitivities (eg. Nut allergy)
What is an antigen? • An external stimuli introduced to the body, evoking an immune response by the body • Honey Bee venom
What is antigenic stimulation? • The body’s physiological response to the antigen • How the body changes in response to being stung • Antigenic stimulation causes a cascade effect on cells
What happens to the bee? • The honey bee’s barbed sting cannot be withdrawn once it has penetrated the skin. • The bee’s only means of escape is to tear away part of its abdomen leaving behind the sting with its venom sac attached. • The muscles of the sting apparatus continue to pulsate after the bee has flown away, driving the sting deeper into the skin and injecting more venom.
Reaction to sting depends on • The amount of venom injected = toxic load, lethal dose (LD50) • State of (un)health of the victims’ immune system • Absence and presence of underlying sensitivity, diseases • Site of sting
Major Constituents of Bee Venomand their activities • Peptides: • Mellitin (haemolysis, cytolysis) • Apamin (neurotoxic, blocks cellular potassium channels) • MCD peptides (=mast cell degranulation) releases histamines and causes allergic reactions
Major Constituents of Bee Venomand their activities • Enzymes: • Phospholipase A (blocks cell membrane function, inhibits blood clotting, drops blood pressure) • Hyaluronidase (faciitates the spread of the inflammation) • Acid phosphatase (contributes to the allergic reaction) • Protease (causes tissue necrosis, cellular death)
Major Constituents of Bee Venomand their activities • Amines: • Histamine (allergic hypersensitivity and inflammation) • Dopamine (affects blood pressure ) • Norepinephrine (affects blood pressure and heart function)
The body’s response • When stung by a bee, the body engages in a sequence of • DOWNSTREAM SIGNALING EVENTS • with a • CASCADE OF EFFECTS • A sequence of cellular responses to antigenic stimulation
Outcomes affected by.. • Genetic diversity • Immune status • Underlying, pre-existing allergies pre-dispose to a more-serious response to bee-stings
Antibodies - IgE • IgA IgE IgG IgM • IgE the immunoglobulin associated with bee sting reactions • Much higher IgE levels are found / present • ** in patients with allergic diseases ** • The anti-IgE antibody “omalizumab” can decrease the risks of anaphylaxis
Effector cells • Mast cells • Mast cells are viewed as key players in IgE-dependent allergies and anaphylaxis • Increased tryptase levels have been detected during acute anaphylaxis in humans • There is a high occurrence of anaphylaxis in patients with high numbers of Mast cells in the body
Inflammatory mediators • Histamines • 4 known histamine receptors • H1 ( & some H2) in anaphylactic bee stings • Understand the use of anti-histamines (cream, tablets) in mild cases
Inflammatory mediators • Some mediators contribute to late consequences of anaphylactic reactions • Delayed reactions (many hours later)
Different expressions • There can be • MILD, • MODERATE, or • SEVERE body reactions, that can be • IMMEDIATE, • DELAYED, or • Bi-PHASIC
Mild to Moderate • Urticaria • Red, itchy • Swelling, puffiness • Spreads… • Eyelids swell closed… • Runny nose • Nauseous
Severe reactions • Can be from a single sting, • Certainly with Mass envenomation • Anaphylaxis ( = hypersensitivity allergic reaction) • Adrenaline (EpiPen) is the only known effective control of acute hypersensitivity reaction
Severe reactions • Mass envenomation occurs with greater than 500 honey bee stings. • This is not an allergic response, it is an anaphylactic response related to a large amount of venom received by the victim. • The dose of sting bee that was calculated to kill (LD50) is • *19 stings per kilogram of body weight*
Bi-phasic & Delayed reactions • A minority of patients exhibit biphasic allergic reactions, • in which signs and symptoms of anaphylaxis recur hours after the early phase of the reaction has waned, • and in some patients late-phase reactions occur without initial hypotension or airway obstruction.
Delayed reactions • “In addition to mast cells and basophils, • macrophages, neutrophils, and perhaps other leukocytes and platelets, also might produce a diverse array of inflammatory mediators during anaphylaxis, • and have the potential to contribute to reactions that might be difficult to treat, protracted in nature, • or biphasic.”
Risks? • Frequent exposure • Elevated risk of anaphylaxis (underlying allergies, medications, diseases) • Prior sting reactions
Risks? • Frequent exposure: • Beekeepers, their families, and neighbours • Foresters, gardeners, emergency personnel, farmers, construction workers, labourers • Outdoor activity
Risks? • Elevated risk of anaphylaxis: • Age (over 40), asthmatic, heart disease • Physical, mental, emotional Stress (lowers Ig’s) • Chronic medications (beta-blockers incl. eye- drops, ACE-inhibitors, possibly some NSAID pain meds) • Skin or Systemic Mast Cell growths (MCT’s)
Risks? • Stress lowers the body’s immune system, • which then impedes the body’s ability to respond appropriately to antigenic stimulation • Eg. stressed then getting ‘flu (=susceptible) • Scientists know that mental, emotional, physical health develops the corresponding healthy immune system • Proven when measuring Immunoglobulin levels with blood tests
Risks? • Site of the sting (where on the body) • Number of stings (how many) • Prior history of (multiple) incidences of being stung • And prior sting reactions, even if not severe, have been found to be an independent risk factor for later, severe, anaphylaxis
What to do? • Work in pairs / have an assistant / let someone know you are working with bees • Be prepared! • Have a plan! • Multiple stings? Seek medical help • Firstline –EPINEPHRINE (EpiPen) • The rest is small stuff, supportive, non-emergency
What to do? • Dress safely and protectively. • Suit up properly. • Preparation • Preparation • Preparation
Can anaphylaxis be beneficial? • “Given that snake (or arthropod) envenomation in the field can result in systemic distribution of the venom, one could argue that systemic IgE-dependent mast cell activation in this setting could both produce the clinical picture of anaphylaxis and also result in the systemic release of mediators (ie. mast cell proteases) that can degrade toxic components of the venom. • In such settings anaphylaxis could be beneficial if it prevents death by envenomation and the unfortunate subject also survives the anaphylaxis.”
Bee venom therapy? • “Although we do not know whether human IgE also can enhance resistance to venoms • (and we imagine that we would have some trouble enlisting volunteers for such a study), • it is tempting to speculate that anaphylaxis induced by small amounts of venom (eg, a single or wasp bee sting) represents only the most extreme and maladaptive end of a spectrum of acquired IgE-mediated immune responses to venom that includes, at the other end of the spectrum, appropriately regulated immune responses that can enhance resistance to such venoms.”
Gr 1 • Skin reactions only • Itching • Flushing, redness • Urticaria (lumps and bumps!) • Angioedema (swelling!)
Gr 2 • Same as Gr 1… plus • Abdomen – Nausea and cramps • Respiratory – Rhinorrhea, hoarseness • Respiratory cont. – Dyspnoea (difficulty breathing) • Cardiovascular - Tachycardia(rise ≥20/min) • Hypotension (≥20 mmHg drop in SBP) • Arrhythmia