Download
1 / 15
150 likes | 317 Views
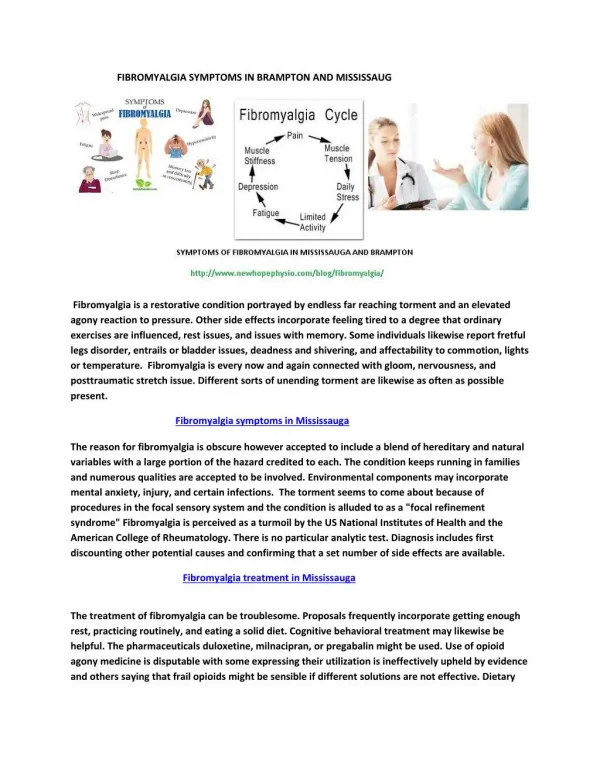
Correlations among Pain Severity, Functional Impairment and Clinical Symptoms in Fibromyalgia. Rebecca L. Ross PhD, RN, PMHNP-BC, Assistant Professor. Background: Fibromyalgia (FM).

E N D
Correlations among Pain Severity, Functional Impairment and Clinical Symptoms in Fibromyalgia Rebecca L. Ross PhD, RN, PMHNP-BC, Assistant Professor
Background: Fibromyalgia (FM) • Prevalence estimated at 2- 5% in the general population (Wolfe et al.1995; Goldenberg et al., 2004; Lawrence et al., 2008) –3.4% in women –0.5% in men –90% women, 10% men • Increases with age • Survey of 2,596 US FM patients(Bennett et al., 2007): –42.4% diagnosed by a rheumatologist –35.4% diagnosed by Family Practitioner or Internist • Second most common disorder seen by rheumatologists (after OA)
Background: FM Burden • Economic Impact • $700 million direct costs in the US (Wolf et al., 1995) • $15.9 billion direct/indirect costs annually (Thorson, 1996) • U.S.Healthcare costs per FM patient annually average $10,199 (White et al., 2008) • Co-morbid Major Depressive Disorder • 30% Cross-sectional Prevalence (Epstein et al., 1999) • 60% Lifetime Prevalence (Epstein et al., 1999)
FM Severity Related to Increased Costs • France, total costs: €7900 =$9,951.28 • direct €910 = $11,46.34 • indirect €6990 = $8,805.75 • Germany, total costs: €7256 = $9140.85 • direct €1765 = $2223.41 • indirect €5491 = $6916.97 • Increased FM severity = Higher total costs (p = 0.003) (Winkelmann et al., 2011)
Background: Major Depressive Disorder (MDD) • Prevalence and Burden: • 2nd leading cause of disability in people ≥5 years worldwide in US (WHO, 2012) • leading cause of morbidity in US (CDC, 2011) • 9.1% lifetime prevalence, approx. 18.8 million Americans (CDC, 2011) • 21% women, 13% men (Kessler et al., 2003) • Economic Impact (Greenberg et al., 2003) • 1990: $43 direct/indirect costs in US • 2000: $52.9 direct/indirect costs in US
Depression- Morbidity Leading cause of disability (YLDs) in world 4th leading contributor to global burden of disease (DALYs) in 2000 Currently, already the 2nd cause of DALYs in the age category 15-44 years for both sexes combined By 2020, projected to reach 2nd place (DALYs) for all ages, both sexes (WHO, 2012)
Background: FM with Co-morbid MDD • FM and Major Depressive Disorder both have a dysregulated HPA axis. (Neeck, 2000, 2002; Nemeroff, 1998; Gold et al., 2002; Tsigos & Chrousos, 2002; de Winter et al., 2003) • Two specific subtypes of MDD have inverse biochemical marker levels.(Gold & Chrousos, 2002) • Atypical depressive episodes (20%-30% prev.) associated with low cortisol levels. • Melancholic depressive episodes (30% prev.) associated with increased cortisol levels.
Biochemical Markers of Depression Subtypes in Fibromyalgia • Sample • Adult females with FM with or without Major Depressive Disorder (MDD) • Setting • Recruited from a tertiary care University Rheumatology FM Clinic in the Pacific Northwest • Sample Size n=62 • FM no MDD n= 7 • FM/ADE n= 31 • FM/MDE n= 24
Methods: Psychometric Measures • Beck Depression Inventory- II (Revised 1973) • Tender-point / Cumulative Myalgic Scale (CMS) • MDD Subtype Screening (DSM-IV) • Hamilton Depression Rating Scale (HDRS) • Flanagan’s Quality of Life Scale (QOLS) • Jenkins Sleep Scale • Fibromyalgia Impact Questionnaire (FIQ)
Statistical Analysis Pearson’s R binomial correlation analyses to examine relationships among: • Individual FM Symptoms: pain severity, stiffness, fatigue • Other clinical characteristics commonly related to FM: pain interference, depression, anxiety, sleep quality, quality of life 3. Functional Capacity physical impairment, functional capacity / overall impact of FM on daily life
Results: Pain Severity • Pain severity (FIQ VAS) highly correlated with: • Physical Impairment(FIQ Subscale: r= 0.508; p<0.001) • Depression (HDRS: r= 0.612; p< 0.001) • Depression (FIQ VAS: r= 0.558; p< 0.001) • Fatigue (FIQ VAS: r= 0.681; p< 0.001) • Stiffness (FIQ VAS: r= 0.667; p< 0.001) • Moderately correlated with: • Sleep (Flanagan’s: r= 0.488; p= 0.001) • Anxiety (FIQ VAS: r= 0.421; p= 0.001)
Results: Physical Impairment • Physical Impairment (FIQ Subscale)highlycorrelated with: • Overall Burden of FM on Daily Life (FIQ Total Score: r= 0.658; p< 0.001) • Anxiety (FIQ VAS: r= 0.637; p< 0.001) • Fatigue (FIQ VAS: r= 0.681; p< 0.001) • Stiffness (FIQ VAS: r= 0.667; p< 0.001) • Moderatelycorrelated with: • Depression (HDRS-17: r= 0.459; p=< 0.001) • Inverselycorrelated with: • Quality of Life (Flanagan’s: r= -0.427; p< 0.001)
Results: Functional Capacity • Overall Impact of FM on Daily Life (FIQ Total Score) highly correlated with: • Pain Severity (FIQ VAS: r= 0.808; p< 0.001) • Depression (FIQ VAS : r= 0.773; p< 0.001) • Depression (HDRS-17: r= 0.663; p=< 0.001) • Anxiety (FIQ VAS: r= 0.637; p< 0.001) • Fatigue (FIQ VAS: r= 0.757; p< 0.001) • Stiffness (FIQ VAS: r= 0.703; p< 0.001) • Moderately with Sleep (Jenkins: r= 0.488; p= 0.001) • Inversely with Quality of Life (r= -0.651; p< 0.001)
Conclusions Findings highlight growing importance of patient-centered individualized treatment for both physical and psychological symptoms of FM. In this time of rising healthcare costs, the concept of systematically identifying which FM symptoms are the most bothersome to patients and focusing treatment accordingly is of special interest to the nursing profession.
Bibliography (To Be Added)