Download
1 / 1
10 likes | 122 Views
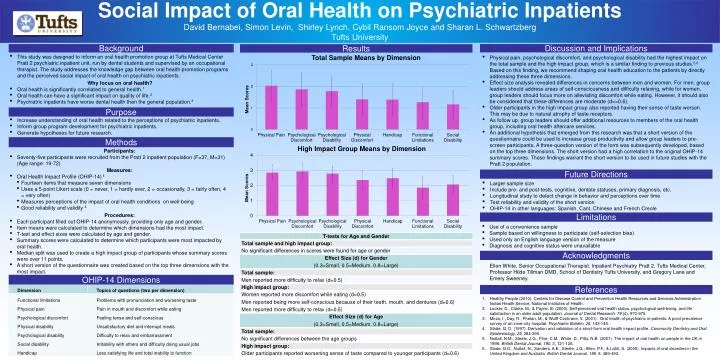
Social Impact of Oral Health on Psychiatric Inpatients. David Bernabei, Simon Levin, Shirley Lynch, Cybil Ransom Joyce and Sharan L. Schwartzberg Tufts University. Background. Discussion and Implications. Results.

E N D
Social Impact of Oral Health on Psychiatric Inpatients David Bernabei, Simon Levin, Shirley Lynch, Cybil Ransom Joyce and Sharan L. Schwartzberg Tufts University Background Discussion and Implications Results • This study was designed to inform an oral health promotion group at Tufts Medical Center Pratt 2 psychiatric inpatient unit, run by dental students and supervised by an occupational therapist. The study addresses the knowledge gap between oral health promotion programs and the perceived social impact of oral health on psychiatric inpatients. • Why focus on oral health? • Oral health is significantly correlated to general health.1 • Oral health can have a significant impact on quality of life.2 • Psychiatric inpatients have worse dental health than the general population.3 • Physical pain, psychological discomfort, and psychological disabilityhad the highest impact on the total sample and the high impact group, which is a similar finding to previous studies.5,6 Based on this finding, we recommend shaping oral health education to the patients by directly addressing these three dimensions. • Effect size analysis revealed differences in concerns between men and women. For men, group leaders should address areas of self-consciousness and difficulty relaxing, while for women, group leaders should focus more on alleviating discomfort while eating. However, it should also be considered that these differences are moderate (d<=0.6). • Older participants in the high impact group also reported having their sense of taste worsen. This may be due to natural atrophy of taste receptors. • As follow up, group leaders should offer additional resources to members of the oral health group, including oral health aftercare services. • An additional hypothesis that emerged from this research was that a short version of the questionnaire could be used to increase group productivity and allow group leaders to pre-screen participants. A three-question version of the form was subsequently developed, based on the top three dimensions. The short version had a high correlation to the original OHIP-14 summary scores. These findings warrant the short version to be used in future studies with the Pratt 2 population. Purpose • Increase understanding of oral health related to the perceptions of psychiatric inpatients. • Inform group program development for psychiatric inpatients. • Generate hypotheses for future research. Methods • Participants: • Seventy-five participants were recruited from the Pratt 2 inpatient population (F=37, M=31) (Age range: 19-72) • Measures: • Oral Health Impact Profile (OHIP-14) 4 • Fourteen items that measure seven dimensions • Uses a 5-point Likert scale (0 = never, 1 = hardly ever, 2 = occasionally, 3 = fairly often, 4 = very often) • Measures perceptions of the impact of oral health conditions on well-being • Good reliability and validity 4 Procedures: • Each participant filled out OHIP-14 anonymously, providing only age and gender. • Item means were calculated to determine which dimensions had the most impact. • T-test and effect sizes were calculated by age and gender. • Summary scores were calculated to determine which participants were most impacted by oral health. • Median split was used to create a high impact group of participants whose summary scores were over 11 points. • A short version of the questionnaire was created based on the top three dimensions with the most impact. Future Directions • Larger sample size • Include pre- and post-tests, cognitive, dentate statuses, primary diagnosis, etc. • Longitudinal study to detect change in behavior and perceptions over time • Test reliability and validity of the short version • OHIP-14 in other languages: Spanish, Cant. Chinese and French Creole Limitations • Use of a convenience sample • Sample based on willingness to participate (self-selection bias) • Used only an English language version of the measure • Diagnosis and cognitive status were unavailable Acknowledgments Ellen White, Senior Occupational Therapist, Inpatient Psychiatry Pratt 2, Tufts Medical Center, Professor Hilde Tillman DMD, School of Dentistry Tufts University, and Gregory Lane and Emery Sweeney. OHIP-14 Dimensions References Healthy People (2010). Centers for Disease Control and Prevention Health Resources and Services Administration Indian Health Service, National Institutes of Health. Locker, D., Clarke, M., & Payne, B. (2000). Self-perceived oral health status, psychological well-being, and life satisfaction in an older adult population. Journal of Dental Research, 79 (4), 970-975. Mirza, I., Day, R., Phelan, M., & Wulff-Cochrane, V. (2001). Oral health of psychiatric in-patients: A point prevalence survey of an inner-city hospital. Psychiatric Bulletin, 25, 143-145. Slade, G. D. (1997). Derivation and validation of a short-form oral health impact profile. Community Dentistry and Oral Epidemiology, 25, 284-290. Nuttall, N.M., Steele, J.G., Pine, C.M., White, D., Pitts, N.B. (2001). The impact of oral health on people in the UK in 1998. British Dental Journal, 190, 3, 121-126. Slade, G.D., Nuttall, N., Sanders, A.E., Steele, J.G., Allen, P.F., & Lahti, S. (2005). Impacts of oral disorders in the United Kingdom and Australia. British Dental Journal, 198, 8, 489-493.