Download
1 / 55
660 likes | 1.89k Views
Antiplatelet and anticoagulant therapy in stroke prevention. Dr Sepehr Shakib Director Clinical Pharmacology Royal Adelaide Hospital. Topics. Stroke basics Risk calculators Lipids and strokes Antiplatelets Clopidogrel Aspirin + dipyridamole Warfarin for AF.

E N D
Antiplatelet and anticoagulant therapy in stroke prevention Dr Sepehr Shakib Director Clinical Pharmacology Royal Adelaide Hospital
Topics • Stroke basics • Risk calculators • Lipids and strokes • Antiplatelets • Clopidogrel • Aspirin + dipyridamole • Warfarin for AF
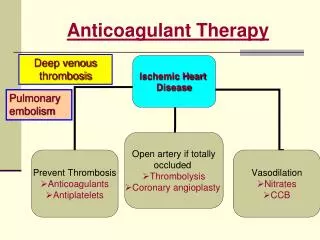
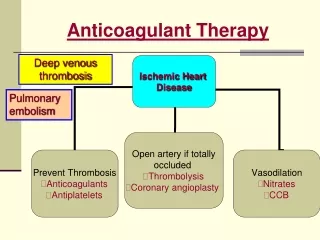
What are the different types of strokes? • Ischemic • Lacunar • Thrombotic • Cardioembolic • Watershed • Hemorrhagic
Ischemic strokes • Lacunar: • Occlusion of deep penetrating branches of arteries • Occlusion caused by microatheroma, lipohyalinosis, hypertension changes • Most caused by hypertension • Account for 20% of all ischemic strokes
Ischemic strokes • Cardioembolic • Strokes from other parts of the vascular tree eg atrial fibrillation, recent MIs, endocarditis, aortic arch etc… • Some caused by lipid accumulation • Thrombotic strokes • Due to development of thrombosis and occlusion of blood vessels supplying brain eg middle cerebral artery
Hemorrhagic strokes • Much more rare and more catastrophic • Caused by: • Hypertension • Amyloid angiopathy • Aneurysms
Hemorrhagic transformation • Development of hemorrhage in large ischemic stroke
Risk • 52 years old • Bp 142/87 • Family history of IHD • LDL 6.4, HDL 0.8 • Has just stopped smoking
Risk Engine Based on UKPDS follow-up data
Relationship between lipids and strokes • BMJ June 2003
Stroke reduction for 1mmol/L reduction in LDL cohort studies 15% reduction in ischemic strokes 19% increase in hemorrhagic strokes
Association between lipids and strokes summary • As your LDL falls • ischemic strokes • ↑ hemorrhagic strokes • Overall benefit depends on the relative balance of absolute risks of ischemic vs hemorrhagic strokes • Even with ischemic strokes get smaller relative reduction in events than IHD • Cf 32% (95% CI 27-36%) reduction in ischemic heart disease events for every 1 mmol/L reduction in LDL
Benefits of lipid lowering in trials • Original evidence from IHD trials • Eg reduction in strokes in 4S and LIPID study • Heart Protection Study first study to demonstrate reduction in strokes in those without IHD (Lancet 2002) • 25% reduction in all strokes
Aspirin • Antithrombotic Trialists’ Collaboration • BMJ 2002 • 287 studies involving 205,000 patients! • Most placebo controlled data related to aspirin
GI bleeding • Meta-analysis 24 RCTs with 66,000 patients • 0.45% annual bleeding rate • OR 1.68 (95% CI 1.51-1.88)
Hemorrhagic stroke risk • 16 trials, 66542 patients • 108 hemorrhagic strokes • Risk 0.05% per year
What about dose of aspirin- efficacy Antiplatelet Trialists Collaboration “There remains uncertainty about such low doses (<75mg) are as effective”
Dose of aspirin- toxicity? • Opinion quite varied from there being no dose dependency to there being one • No direct comparison of doses • Small adverse event rate • Differences in background populations in different studies
Am J Cardiol 2005 • 31 trials • 192,036 patients • Looked at low (<100mg), moderate (1-200mg) and high dose (>200)
Bleeding risk There appears to be dose dependency Toxicity is substantial even at low dose
Aspirin summary • Effective at reducing rate of recurrent stroke • Even small doses associated with risk of bleeding • Mainly GI bleeding but some intracerebral • Benefit outweighs risk in patients with previous stroke • There appears to be increased toxicity at increased doses
Clopidogrel • CAPRIE study • Clopidogrel 75mg vs aspirin 325mg • History of stroke, MI, or peripheral vascular disease • 19,185 patients
Clopidogrel efficacy 5.8% 5.3%
Clopidogrel toxicity * p<.05
Aspirin + Dipyridamole • Antithrombotic Trialists Collaboration 2002 • 6% non-significant reduction in strokes with addition of dipyridamole to aspirin • Systematic review of 25 studies, involving 10,404 patients
2700 patients randomised to any dose of aspirin +dipyridamole SR 200mg twice daily Open label ESPRIT study
Esprit results • Fewer strokes with aspirin + dipyridamole • Fewer hemorrhages with aspirin + dipyridamole (??) • Systematic review of 6 studies shows reduction in recurrent events
Antiplatelet therapy Which is the ideal antiplatelet? • Stroke 2008 meta-analysis: addition of dipyridamole to aspirin: ‘robust benefit’ • Editorial: “…considering the 40 times difference in cost and the discrepancies noted above, such benefit is uncertain and, judging by the data, far from robust”
PROFESS • Recent ischemic strokes • Randomised to clopidogrel or asa+dip • 20,000 patients for 2.5 years • Non-inferiority design
Primary outcome- recurrent stroke Hazard Ratio for Aspirin–ERDP 1.01 (0.92–1.11)
Antiplatelet key messages • Aspirin is antithrombotic of choice in primary stroke prevention when CV risk is high • Aspirin, aspirin+dipyridamole or clopidogrel are main antiplatelet cfhoices in secondary stroke prevention • Choice depends on circumstances (PBS criteria, intolerances)
Risk of stroke with AF • Risk highest with valvular AF • All other stratification tools refer to non-valvular AF • There are numerous different risk stratification tools which rely on different risk factors
CHADS2 Score • National Registry of Atrial Fibrillation • JAMA 2001 • Subsequently validated in different studies
Benefit of antithrombotic therapy • Warfarin reduces risk of stroke by 70% • Aspirin reduces risk by 30% • Less effect on large disabling strokes • Aspirin + dipyridamole- very limited data • Clopidogrel- no data • Aspirin + clopidogrel- not as good as warfarin ? Better than aspirin