Download

1 / 40
410 likes | 681 Views
Anticoagulant therapy. Background Cost Benefit Complication. External(F7)15s Internal(F12)1 to6minute Result> prothrombin activator prothrombin (F2)>thrombin>fibrinogen(F1)>fibrin. Clot formation: fibers+platlet+red cell+plasma

E N D
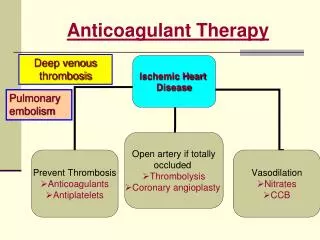
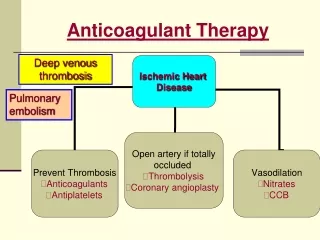
Anticoagulant therapy • Background • Cost • Benefit • Complication
External(F7)15s • Internal(F12)1 to6minute • Result>prothrombin activatorprothrombin(F2)>thrombin>fibrinogen(F1)>fibrin
Clot formation: fibers+platlet+redcell+plasma • Restrictive clot formation:antithrombin3+thrombin(12_20minute) • Clot retraction:30to60minute • Clot leases During 24hours TPA release injury endothelium and activated plasminogen>plasmin(fibrinolisin)>leases: Fibrinogen,prothrombin,F5,F7
Anticoagulant drugs: 1__HEPARIN • UFH or LMWH ?
Heparin(UFH) release from mast cell basophile around capillary and concentration lung and liver • UFH: heterogenus mixture glycosaminoglycant with MW3000 to30,000 only one third is active anticoagulant with bind antithrombin and increase activation 1000X for neutralize troponin and F9,F10,F11,F12
Half life: dependent dose 25U/kg 30min • 100u/kg60min • 400u/kg150min • aPTT only sensetive heparin range1.0-0.1u/ml • More than 1.ou/ml withACT(hemotec parker-itcedisonmedtronic)350-375 secischemic complication at 7days are 34%lower than thy were ACT171-295 • Heparin doses70 to 100iu/kg and target act250-350seconds but with GP2b/3a inhibitor 40-70iu/kg target ACT 200to 250sec
Low molecular weight hepaarins(LMWH) • Manifactured from UFH withchemical or enzymatic fragment s one third size • Binds less readily to plasma protein, more resistant to neutralization by platelet F4(half life4hours),less effect on platelet function • Relatively selective inactivation factor xa
Complication: • Bleeding,predispose with increase risk was :age ,alcohol,aspirin, ,renal failure, serious concurrent illness. LMWH risk more increase in RF • Prothaminesulfat dose not comletly effective in reverse antifactorxa activity inLMWH
Thrombocytopenia:tow type • Begins 4-14 days exceptions are in patient received heparin the past three month.50% drop in platelet count • Dose depended 15% benign and self limited • Immune form(HIT) paradoxically cause serious arterial and venous thrombosis(HITT) mechanism interaction antibody IgG with complex of heparin and platelet factor4 is released on activation
Declininplatlet count in HIT is usually:50;000 to 60,000/mm3 • Immune –mediated HIT is not heparin dose dependent even heparin flushes • HIT no single definitive laboratory test(platlet activation assay, serotonin release assay) • When HIT is suspected heparin discotinude but HIT is associated with marked hypercoagulable state with 30to 50% thrombosis in 30 days after diagnosis
Threatment HITT • No LMWH because strong cross reaction with HIT • No warfari • Tow direct Thrombin inhibitors :lepirudin and argatroban and pentasacaridefondaparinux(binding platlet factor4)
2-Warfarin(coumadin) • Vitamin K antagonist Vkh2 is cofactor forF2(prothrombin)F7,F9,F10 • Mean plasma half life` 40hours metabolism is affected allelic variant of P450,CYP2C9 homozygous for active alleles with low warfarin dose and high bleeding complication and polimorphism in VK epoxidreductase(VKOR)gene also influence anticoagulant respone • Drugs: propranolol,amiodaron,clofibrate,cimetidine……increase warfarin levels and cholestyraminerifampin …..decreas high VK in diet(nutritional supplement)
Loading doses of warfarin should not be used • Because:VK dependent factors have different half life F7 shortest initial increase INR withsevere F& deficiency state while still failing to provide antithrombotic effect. • Reduction in plasma level protein C (VK dependent anticoagulant with shortest HL) Lead to transient paradoxical hypercoagulated state.