Download
1 / 53
530 likes | 654 Views
Jefferson Heart Institute 925 Chestnut Street. Referring Physician. Name of physician Office Address Pride Communication More referrals. “Carbon Copy”. Interested physicians Office Address Pride Communication More referrals. Reason for the visit (a.k.a., chief complaint).

E N D
Referring Physician Name of physician Office Address Pride Communication More referrals
“Carbon Copy” Interested physicians Office Address Pride Communication More referrals
Reason for the visit Pulmonary hypertension evaluation Elevated pulmonary artery pressure by echocardiogram Elevated pulmonary artery pressure by right heart catheterization
History of Present Illness W.H.O. Functional Class W.H.O. Group Drugs trialed and response to therapy Relevant family history Relevant testing
Symptoms of PH • Dyspnea Fatigue • Syncope Edema • Dizziness Chest Pain Non-specific nature of complaint can lead to: • Confusion with other conditions • Delayed diagnosis Gaine et al. The Lancet, 1998. 352; 719
W.H.O. Functional Classification Class I: Patients with PH but without resulting limitation of physical activity. Ordinary physical activity does not cause undue dyspnea or fatigue, chest pain or near syncope. Class II: Patients with PH resulting in slight limitation of physical activity. They are comfortable at rest. Ordinary physical activity causes undue dyspnea or fatigue, chest pain or near syncope. Class III: Patients with PH resulting in marked limitation of physical activity. They are comfortable at rest. Less than ordinary physical activity causes undue dyspnea or fatigue, chest pain or near syncope. Class IV: Patients with PH with inability to carry out any physical activity without symptoms. These patients manifest signs of right heart failure. They are comfortable at rest. Dyspnea and/or fatigue may even be present at rest. Discomfort is increased by any physical activity. (Syncope)
W.H.O. Classification - 2008 2. Pulmonary hypertension owing to left heart disease 2.1 Systolic dysfunction 2.2 Diastolic dysfunction 2.3 Valvular disease 3. Pulmonary hypertension owing to lung diseases and/or hypoxemia 3.1 Chronic obstructive pulmonary disease 3.2 Interstitial lung disease 3.3 Other pulmonary diseases with mixed restrictive and obstructive pattern 3.4 Sleep disordered breathing 3.5 Alveolar hypoventilation disorders 3.6 Chronic exposure to high altitude 3.7 Developmental abnormalities 4. Chronic thromboembolic pulmonary hypertension (CTEPH) 5. Pulmonary hypertension with unclear multifactorial mechanisms 5.1 Hematologic disorders: myeloproliferative disorders, splenectomy 5.2 Systemic disorders: sarcoidosis, Langerhans cell histiocytosis: lymphangioleiomymatosis, neurofibromatosis, vasculitis 5.3 Metabolic disorders: glycogen storage disease, Gaucher disease, thyroid disorders 5.4 Others: tumoral obstruction, fibrosing mediastinitis, chronic renal failure on dialysis
Past Medical History W.H.O. Group 1 Heritable Collagen vascular disease HIV Portal hypertension Anorexigenic agents Hemoglobinopathies
Past Medical History W.H.O. Group II Left heart disease W.H.O. Group III Lung diseases and/or hypoxemia W.H.O. Group IV Chronic thromboembolic PH W.H.O. Group V Unclear multifactorial mechanisms
Heritable pulmonary arterial hypertension Dresdale, 1953 reported family NIH Registry, 1987: 6% with one or more affected family members Autosomal dominance Fetal wasting Genetic anticipation Incomplete penetrance
Idiopathic PAH - Epidemiology • Female • Young to middle age • NIH Registry, 1991
Congenital Heart DiseaseEpidemiology Shear stress from increased pulmonary blood flow Increased pulmonary artery pressures Majority of unrepaired truncus arteriosus develop PH Large VSD, 50% develop PH ASD, 10% develop PH Eisenmenger’s syndrome Medical or surgical therapy effective
Connective Tissue DiseasesEpidemiology • Limited systemic sclerosis • SLE, MCTD, RA, Sjogren’s
HIVEpidemiology 0.5% prevalence– no decline since HAART Occurrence depends upon length of infection, not CD4 count or prior opportunistic infections
Portopulmonary HypertensionEpidemiology • 2-6% prevalence in cirrhotics, higher in liver transplant candidates (8%) • Risk increases with duration of portal hypertension • High cardiac flow states and LV diastolic dysfunction complicate PH
Pulmonary Hemodynamic Scenarios in the Setting of Portal Hypertension Type MPAP PAOP CO PVR TPG I. Hyperdynamic, high flow state ↑ n ↑ ↓ n II. Increased pulmonary venous vol. ↑ ↑ ↑ ↓ n III. Portopulmonary hypertension Pulmonary vascular obstruction;normal volume ↑ ↓ ↑ ↑ ↑ Pulmonary vascular obstruction; ↑ ↑ ↑ ↑ ↑excess volume M Krowka. Medscape Cardiology 2006
Associated Drugs and ToxinsEpidemiology • Definite: • Appetite suppressant drugs (anorexigens) • Fenfluramine and dexfenfluramine • Aminorex • Toxic Rapeseed Oil • Likely: • L-tryptophan • Methamphetamine • Cocaine
HemoglobinopathiesEpidemiology • Sickle cell disease • PH 10-30% • Yearly echocardiogram • 50% - 2 year mortality with PH • Thromboembolic disease • Restrictive pulmonary disease • Left heart disease • Homozygous beta-thalassemia • Hereditary spherocytosis
Chronic ThromboEmbolic Pulmonary Hypertension (CTEPH)Cumulative Incidence Historically considered rare: 0.1-0.5% of acute, non-fatal pulmonary embolism: Fedullo PF et al. N Engl J Med 2001 6 months 1.0% 12 months 3.1% 24 months 3.8% Pengo V, et al NEJM 2004
Past Surgical History Lung resection Thyroidectomy Splenectomy CABG Cardiac valve repair/replacement Repair of congenital heart defect
Family History Pulmonary hypertension CHF/sudden cardiac death at a young age Sarcoid Connective tissue disorders Clotting disorders – DVT, PE, CVA
Social History Tobacco ETOH Recreational Drugs methamphetamines Cocaine IVDU Prescription diet pills Bush tea Pets (birds) Social Network – “Friends and Family”, not “Verizon”
Allergies /Adverse Reactions Beware of hypotensive response to vasodilators CCBs Nitrates Sildenafil
Medications Nitrates Calcium channel blockers Warfarin Beta blockers Oxygen Diuretics Digoxin
Medications ERAs (Bosentan) Hepatotoxins – monitor LFTs, Hgb Glyburide may increase risk of hepatoxicity Cyclosporine Ketoconazole Statins Warfarin (Ambrisentan*)
Medications PDE V Inhibitors • Sildenafil (Revatio) • Tadalafil (Adcirca)
Medications Prostacyclins Parenteral Route of administration Inhaled ng/kg/minute mcg/dose ml/24 hrs frequency
Review of Systems Neurologic: Headache, prior TIA/CVA, lightheadedness or syncope HEENT: Epistaxis, dry eyes, dry mouth, oral ulcers. CV: Anginal quality chest pain, orthopnea, PND, palpitations, peripheral edema Rheumatologic: Joint pain or swelling, Raynaud’s phenomenon GU/Gyn: Hematuria, Gravida : Para (spontaneous abortions) GI: Liver disease, dysphagia, heartburn, hematemesis, varices or hemorrhoids, ascites
Review of Systems Hematologic/Lymphatic: DVT, PE, CVA, TIA (hypercoaguable state) swollen lymph glands (Sjogren’s, sarcoid) Dermatologic: Rashes, skin lesions, painful ulcers on fingertips. Psychiatric: Confusion, memory loss, depression, anxiety HIV risk factors: Blood transfusions, known contacts, HIV serum test (date) Sleep: Snoring, witnessed apneas, restless sleeper, awakens unrefreshed, daytime hypersomnolence
Physical Examination Jugular venous distention at 45o Widened split S2 Loud pulmonic valve closure (P2) TR murmur Right ventricular heave, PA pulsation Enlarged, pulsatile liver – hepatojugular reflux Peripheral edema, ascites Skin/Mouth: Telangiectasias, spider hemangiomas *Infusion catheters and site problems
Guidelines for evaluating pulmonary hypertension Barst, R. J. et al. J Am Coll Cardiol 2004
IVS RV LV RA LA Laboratory evaluation
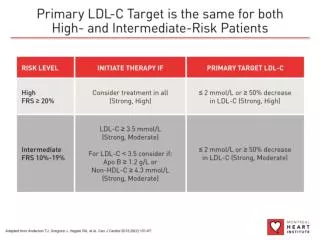
Impression 1. (Suspected) Pulmonary (arterial) hypertension (with/without) right ventricular dysfunction due to __________: W.H.O. Functional Class 1 - 4 2. Other conditions contributing to cardio-respiratory complaints
Recommendations and Plan Defend you reason for your assessment Defend your reason for testing ordered Defend your reason for medical therapy One paragraph per “Impression #” Write so that the referring doctor will understand Write so you may use this note as a reminder for what you wish to do at next visit. Jefferson Heart Institute – follow-up
Tools for Patients Cardiology nurses for RHC teaching PH literature tearouts Teaching aides – RHC booklets Parenteral infusion CDs Inhalation device models