Download
1 / 59
590 likes | 683 Views
THE ENDOCRINE SYSTEM. Purpose : Communication Nature : Slow, not specific Regulates : growth, metabolism, reproduction, autonomic functions. hormone. Cell A. Cell A. Cell A. Cell B. hormone receptor. blood. DEFINITIONS. HORMONE. Cell B. PARACRINE AGENT. AUTOCRINE AGENT.

E N D
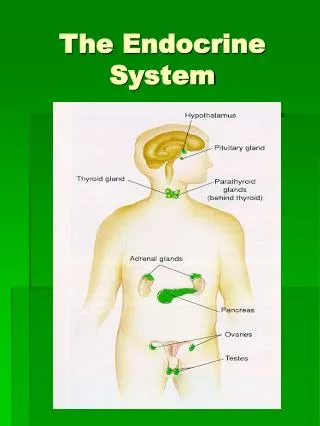
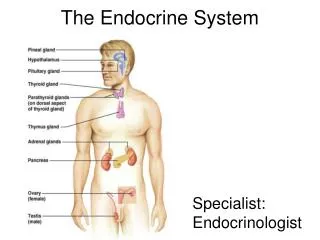
THE ENDOCRINE SYSTEM Purpose: Communication Nature: Slow, not specific Regulates: growth, metabolism, reproduction, autonomic functions
hormone Cell A Cell A Cell A Cell B hormone receptor blood DEFINITIONS HORMONE Cell B PARACRINE AGENT AUTOCRINE AGENT
CHEMICAL NATURE OF HORMONES Amines: epinephrine, norepinephrine, dopamine, T3, T4 Peptides and proteins: insulin, glucagon, TSH, TRH, (many others) Steroids: testosterone, estrogen, progesterone, cortisol, aldosterone
Amines, proteins and peptides (except T3, T4): • Water soluble • Can’t cross cell membranes • Bind to receptors on cell surface • Effects usually rapid and transient • Not effective when ingested • Steroids and T3, T4: • Not water soluble (need a carrier in blood) • Can cross cell membranes • Bind to receptors in the cytoplasm or on DNA • Act primarily by initiating gene transcription • Effects usually slow and sustained • Effective when ingested, can also be applied topically
Regulation of Thyroid Hormone release
TSH causes: • Uptake of iodine • Synthesis of thyroglobulin • Iodination of thyroglobulin • Uptake of colloid into thyroid cell • Secretion of T3/T4 from thyroid cell • Increase in the size and number of thyroid cells
T3 Cell membrane T3 cytoplasm Nuclear membrane gene T3 receptor
EFFECTS OF THYROID HORMONES • Increased O2 consumption/metabolic rate • -Increased size of mitocondria • - Increased expression of respiratory enzymes • - Increase Na+/K+ ATPase • - Increased proteins for growth and maturation • Increased expression of b-adrenergic receptors • Required for brain development
IODINE REQUIREMENTS (mg/kg/day) Infants (10-12 mo) 15 Children (1-6 yr) 6 School children (6-12 yr) 4 Adults (12+ yr) 2 Pregnant and 3.5 lactating women
DIETARY SOURCES OF IODINE (ug/g) Fish (fresh water) 17-40 Fish (marine) 163-3180 Shellfish 308-1300 Meat 27-97 Milk 35-56 Eggs 93 Grain 22-72 Fruits 10-29 Legumes 23-36 Vegetables 12-201
IODINE DEFICIENCY • Leading cause of brain damage worldwide (13% of world • population) • Another 39% at risk • 130 developing countries affected • particularly problematic in pregnant women (iodine • required for fetal development) • even mild cases with no symptoms can result in a • decrement of 15 IQ points
How do you know if someone is iodine deficient? • Increased thyroid size • Increased serum TSH levels
Regulation of Thyroid Hormone release
Insufficient dietary iodine Inability of thyroid to make T3/T4 Reduced serum T3/T4 Less T3/T4 inhibition of anterior pituitary TSH synthesis Increased serum TSH Increased thyroid growth (goiter) Increases efficiency of the thyroid for T3/T4 production
CONSEQUENCES OF IODINE DEFICIENCY Fetus Abortions/stillbirths Congenital abnormalities Increased perinatal mortality Neurological deficits (cretinism) Mental and growth retardation Psychomotor defects Neonates Goiter Hypothyroidism Children Goiter Hypothyroidism Impaired mental function Retarded growth Adults Goiter Hypothyroidism Impaired mental function
A Public Health Story Early 1900’s goiter was highly prevalent in the Great Lakes and Northwest regions of the US 1924: Michigan department of Health does survey in 4 counties. 39% of children have goiter. Begins campaign for iodized salt. 1928: Same counties resurveyed. Goiter down by 75% 1951: Goiter prevalence less than 0.5% 1993: Universal Salt Iodization Program started (WHO). Global rates of goiter, cretinism and mental retardation are declining rapidly.
Why salt? • Cheap (0.05 US$ per person per year) • Widely available • Consumed throughout the year
Hyperthyroidism – Grave’s Disease • most common cause of hyperthyroidism • autoimmune disorder • Antibodies that stimulate TSH receptor • increased T3/T4 levels • goiter (enlargement of the thyroid)
Regulation of Thyroid Hormone release Antibodies that stimulate TSH receptor
Grave’s Disease - Symptoms • Hypermetabolic state • Excess sympathetic nervous activity • Psychological symptoms • Overactivity of muscles retracting eyelids: increased staring, decreased blinking • Exopthalmus (protruding eyes) • Increased gut motility (diarrhea)
Grave’s Disease - Treatment • Destroy gland • Surgery • Radioactive Iodine • Block T3/T4 synthesis • Thiouricil: inhibits peroxidation of thyroglobulin • Lithium (blocks TSH signal transduction pathway)
Hypothyroidism • inadequate production of thyroid hormone • Primary • Ablation of thyroid by surgery/radioisotopes • Hashimoto’s thyroiditis • Autoimmune • idiopathic • Secondary • Lack of TSH
Hypothyroidism – Symptoms (adult onset) • Decreased metabolic state • Cold intolerance, fatigue, hypothermia, weight gain • Decreased sympathetic activation • bradycardia • Slowing of intellectual and motor activity • Forgetfulness, apathy, even dementia • Decreased gut motility (constipation) • Myxedema
Myxedema • Accumulation of mucopolysaccharides and fluid in tissues • Facial puffiness • Edema • Hoarseness • Joint stiffness • Nerve compressions/parathesias • Pleural, cardiac, and peritoneal effusions
Hypothyroidism – Symptoms (childhood onset) • Cretinism (lack of T3/T4 in childhood) • impaired development of skeletal, nervous system • mental retardation • historically, dietary; iodine supplementation eliminates
Effects of growth hormone • Bone growth • Protein synthesis • Anti-insulin effects • Results in: • Decreased adiposity • Increased lean body mass • Increased organ size and mass • Increased plasma glucose concentrations
Lengthening occurs at epiphyseal plates • At puberty, epiphyseal plates close • After puberty, bones can get wider, but • not longer
Acromegaly • Caused by increased growth hormone secretion • Usual cause is a tumor of the GH secreting cells • of the anterior pituitary
Alterations in GH secretion • Oral glucose challenge usually decreases GH levels to • undetectable, but not in acromegaly (used in diagnosis) • Response to GHRH is increased • Hypoglycemia and arginine both increase GH (same as normal) • Somatostatin lowers GH but not to normal
Effects • Increased bone muscle and connective tissue growth • Increased incidence of diabetes • Effects of tumor mass • Headaches • Vision impairment, particularly peripheral vision • (optic nerve runs near the anterior pituitary) • Effects resulting from loss of anterior pituitary • hormones due to compression of the pituitary • by tumor mass (loss of FSH and LH: amennorhea in women, • impotence in men and reduced secondary sex characteristics in men)