Download
1 / 56
580 likes | 1.08k Views
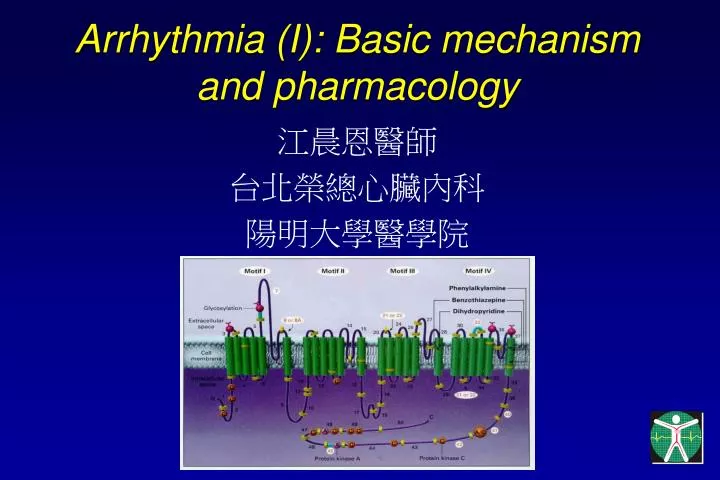
Arrhythmia (I): Basic mechanism and pharmacology. 江晨恩醫師 台北榮總心臟內科 陽明大學醫學院. Basic Electrophysiology. Calcium channels. Potassium channel. Atrial & Ventricular myocytes. SA nodal cells. Ionic currents for ventricular myocytes. Koch’s Triangle. Mechanisms of arrhythmia.

E N D
Arrhythmia (I): Basic mechanism and pharmacology 江晨恩醫師 台北榮總心臟內科 陽明大學醫學院
Atrial & Ventricular myocytes SA nodal cells
Mechanisms of arrhythmia • Abnormality in impulse formation • Abnormal automaticity • Triggered activity (triggered automaticity) • Early afterdepolarization (EAD) • Delayed afterdepolarization (DAD) • Abnormality in impulse conduction • Reentry
Normal Automaticity Pacemaker current (If) + L-type Ca current + T-type Ca current
具有自發性放電功能之傳導組織 • 竇房結 • 房室結 • 浦頃氏纖維 * 心房及心室肌肉正常時不具自發性放電功能
Abnormal automaticity • Myocardial ischemia • Electrolyte imbalance
Phase 2 EAD: Ca2+ window current or Na+-Ca2+ exchange current Phase 3 EAD: Na+ window current Early Afterdepolarization (EAD): LQTS
Delayed Afterdepolarization (DAD): Digitalis Intoxication Na+-Pump Na+(i) CA2+(i) Intracellular Ca overload Depolarization Na-Ca exchanger 1 positive charge into cell Non-specific cation channel Depolarization
Reentry • Anatomical reentry (curable by RFCA) • Sinus nodal reentrant tachycardia (SART) • Intra-atrial reentrant tachycardia (IART) • AV nodal reentrant tachycardia (AVNRT) • AV reciprocating tachycardia (AVRT)(WPW) • Common atrial flutter (AFL) • Monomorphic ventricular tachycardia • Ischemic: scar, aneurysm • Idiopathic LVVT • Bundle branch reentry VT (BBRT)
診斷 • 自己觸診脈搏 • 普通心電圖 • 二十四小時心電圖 • 事件紀錄器(可紀錄一星期) • 運動心電圖(較少診斷效果) • 心導管檢查(具輕度危險性)
Classification of Antiarrhythmic Drugs • Singh-Vaughan Williams Classification • 1971, 1981, 1984 • Sicilian Gambit • 1991, 1993, 199?
Class IA: QT prolongation (also block K channel) Class IB: QT shortening Class IC: QT unchanged Class III: QT prolonged
Vaughn-WilliamsClassification of Antiarrhythmic agents • Class 1: Na channel blockers • IA: quinidine, procainamide, disopyramide • IB: lidocaine, mexiletine, tocainide • IC: propafenone, flecainide • Class II: beta-blockers • Class III: K channel blockers • Sotalol, amiodarone, ibutilide, azimilide • Class IV: calcium channel blockers (CCB) • Non-nifedipine: verapamil, diltiazem
Mechanisms of antiarrhythmic action Excitable gap • Prolong refractory period (Class III drugs) • If the excitable gap is short: A. fib • Block conduction directly (Class I drugs) • If the excitable gap is long: A. flutter
Other antiarrhythmic agents • Digitalis • Mechanisms (unrelated to Na pump) • Decrease sympathetic outflow • Increase parasympathetic tone • Indicated in patients with CHF • Slow onset, long half-life (30-40 hours)
Other antiarrhythmic agents • Adenosine • A1 receptor in cardiac tissue (A2 in vasculature) • A1R >>> Gi Protein • Open Kach.ado (ligand gated potassium channel) • Shortening of APD (atrium) • Hyperpolarization of resting membrane potential • Inhibit adenylyl cyclase (Anti-adrenergic effect) • Very short-acting (T1/2: 1.5 s) • Rapid blockade of AV node conduction • 6,12, 12 mg iv bolus • Decrease dose in patients with dipyridamole • Ineffective in patients with theophylline • Contraindicated in patients with asthma • Treatment of choice in patients with PSVT
Drugs for Blocking Conduction(Use-, Frequency-dependence) • Slow conduction (Ca2+-channel mediated, SAN, AVN) • Class IV: Calcium channel blockers (CCB)(except dihydropyridine group: nifedipine, etc) • Class II: -blockers • Digitalis, adenosine • Fast conduction (Na+-channel mediated, atrial and ventricular myocardium, His-Purkinje system, and accessory pathway) • Class IA, IC: atrial and ventricular myocardium • Class IB: ventricular myocardium
Drugs for Prolonging Refractoriness(Reverse use-dependence) • SAV, AVN • Class IV: CCB (except dihydropyridine group: nifedipine, etc) • Class II: -blockers • Vagotonia: edrophonium, vagal maneuvers • Digitalis • Atrial and ventricular myocardium, and accessory pathway • Class IA and Class III, Class IC (mild) • Amiodarone: devoid of reverse-use dependence
Reverse use-dependence Amiodarone Sotalol
VPD Hypothesis • Post MI • VPC > 10/ hour: high risk • Class IC drug (flecainide, encainide), very effective in suppressing post-MI VPCs • CAST study • Class IC 2.6 folds higher risk of death • Class IC: absolute contraindicated in patients with a history of MI
Proarrhythmic effects • Class IA • Acceleration of ventricular rate in AF and AFL • Quinidine syncope • Acquired LQTS: torsade de pointes • Class IC • Acceleration of ventricular rate in AF and AFL • Mimicking VT • VT (CAST study) • Class III • Reverse use-dependence: LQTS
Incessant slow VT (proarrhythmic effect by class IC drug in IHD)