Download
1 / 25
250 likes | 508 Views
Long Term Conditions Strategy. Andrew Hindle: Commissioning Lead for LTC Dr Liz Pope: Clinical Lead for LTC Joanne Gutteridge: Project Lead for LTC. Building on achievements. COPD LES Early supported discharge for stroke patients Virtual Wards pilot Community neurological team.

E N D
Long Term Conditions Strategy • Andrew Hindle: Commissioning Lead for LTC • Dr Liz Pope: Clinical Lead for LTC • Joanne Gutteridge: Project Lead for LTC
Building on achievements • COPD LES • Early supported discharge for stroke patients • Virtual Wards pilot • Community neurological team
Patient, public and carer engagement • Service users and carers involved in developing pathways, re-design of services including: • Patient Representatives on each of the LTC local implementation teams • Workshops and consultation on the neurology strategy and dementia strategy • Dudley Health Care Forum • Dudley Stroke Association
LTC challenges in Dudley • Increasing numbers of people with LTCs • Ageing population • Unhealthy lifestyles manifest into LTCs • DH suggest that 70% of total health care budget is related to care of people with LTC’s (potential huge savings to be made)
LTC context in Dudley • Two thirds of over 75’s have a LTC • Over 35,000 carers in Dudley • One in five people in Dudley report having a LTC which limits daily life • Increasing gaps between the most and least deprived wards in Dudley therefore this strategy adjoins to Health Inequalities Strategy
LTC Board and LITs • The following LTC’s have been identified as the most significant for focus and LIT’s established that report to the LTC Board: • CHD • Diabetes • Neurology • Renal • Respiratory • Stroke • Cancer • Dementia
LTC Structure PCT Strategic Plan LTC Strategy Urgent Care PEC LTC Board Planned Care Board Dudley Cluster Board LTC Board Lead – Dr Liz Pope LTC Strategic Commissioner – Andrew Hindle CANCER Lead Commissioner Caroline Salmon Clinical Lead Dr Tony Collins STROKE LIT Lead Commissioner Derek Hunter Clinical Lead Dr Liz Pope CHD LIT Lead Commissioner Joe Gutteridge Clinical Lead Dr Rosie Thorns RENAL LIT Lead Commissioner Joe Gutteridge Clinical Lead Dr Kumar DIABETES LIT Lead Commissioner Joe Gutteridge Clinical Lead Dr Helen Moran DEMENTIA Lead Commissioner Andrew Hindle Clinical Lead Dr Liz Pope RESPIRATORY LIT Lead Commissioner Andrew Hindle Clinical Lead Dr Mark Hopkin NEUROLOGY LIT Lead Commissioner Andrew Hindle Clinical Lead Vacant
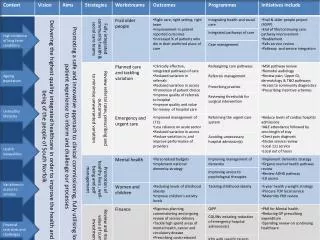
LTC QIPP Priorities • Our vision is for services that: • better identify and manage risk • offer generic strategies for people with multiple conditions • prevent disease progression • support self care • develop personalised care plans in a partnership between patients and clinicians • exploit assistive technology, e.g. telehealth, wherever possible and appropriate • are delivered through a highly skilled workforce well trained and educated in the particular needs and circumstances of people who live often with long-term and life limiting conditions
Table 2 - Actual versus Modelled Prevalence - 2009/10 Sources: QOF Data for prevalence register sizes, Doncaster QOF Analysis Tool for modelled prevalence 1 Source: APHO Disease Prevalence Model Projections (http://www.apho.org.uk/resource/view.aspx?RID=48308 Accessed January 2010), based on ONS mid-year 2006 population projections applied to PCT populations.
Actions to address under diagnosis in Dudley • QOF figures for LTC’s sent to practices and action plans may be requested where below national average • Respiratory LIT to implement education and training on asthma to increase identification • Vascular check • “Think Glucose” • COPD “missing millions” pilot
Goals and actions: Stroke • Best Practice payment scheme developed to ensure more patients spend 90% of their admission time on a stroke ward and more patients scanned on or within 1 hour • To develop regular reviews to ensure better follow up and goal planning for stroke patients • To embed the early supportive supported discharge scheme as a permanent solution • To develop better links with West Midlands Ambulance Service re “FAST” for handover of patients in acute and alerted for arrival in A&E/EAU
What can you do? Follow the annual review protocol as detailed in the Stroke guidelines
Goals and actions: Cancer • To develop and deliver social marketing campaigns to raise awareness of 6 cancers (breast, cervical, skin, bowel, prostrate, lung) to increase cancer awareness, to manage at an earlier stage of diagnosis and increase 1 year survival • To embed the breast screening age range is extended from 47-73 to decrease breast cancer mortality
Goals and actions: Neurology • To reduce neurology out-patient activity by 5% per year over the next 5 years (develop community neurology team) • To develop Multiple Sclerosis pathway for Disease Modifying Therapies at Dudley Group of Hospitals rather than at University Hospital Birmingham where treatment is currently located • To commence a pilot of a MDT clinic with consultants and community neurology team
What can you do? Refer known neurological patients to the community neurological team if they need ongoing input from specialist nurse, physio, OT, or specialist pharmacist
Goals and actions: CHD • To re-design current cardiology out patient services provision to increase capacity, by delivering a primary care based solution for non-complex cardiac conditions • To commence a 6 month RCT pilot assessing the economic value of using Tele-health for HF patients. • To undertake an AF LES which focuses on the identification, stroke risk stratification and appropriate treatment to reduce strokes. • To develop a hypertension pathway • To conclude pilot of Electrocardiogram and event monitoring within practice December 2010
What can you do? Actively call patients in for the Vascular Checks Opportunistically screen for hypertension Improve management of known hypertension patients Sign up to the AF LES
Goals and actions: Respiratory • To implement as part of the National COPD Strategy a ‘Missing Millions’ (previously undiagnosed COPD) pilot. Audit of 800 patients via GP surgeries, community pharmacists, Dudley Stop Smoking Service • To implement the new NICE guidelines for COPD Mild, Moderate, Severe and Very Severe • To improve diagnosis of asthma in Dudley via an education and training programme • To take forward an application via SHA End of Life workforce projects for an end of life care lead/nurse for COPD • To redesign of pathways for children with allergy, asthma and eczema to improve services and patient outcomes and reduce costs
What can you do? Participate in the Missing Millions pilot Actively recall all COPD patients for COPD LES evaluation
Goals and actions: CKD • To increase home therapy for renal placement therapy (via QIPP and West Midlands Renal Network) • To implement an end of life pathway and include a conservative management pathway • To reduce the prevalence gap of CKD via working with practices and ensure action plans are in place to address the prevalence gaps
Goals and actions: Diabetes • To redesign Diabetes pathways and LES • To take forward the ‘Think Glucose’ scheme as part of a national CQINN scheme to reduce LOS in hospitals by education and training to non-specialist medical teams for identification of diabetes and timely referral to specialist diabetes teams • To embed the Foot Care pathway for early identification of complications and reduce major surgery including amputations
What can you do? Diabetes LES Vascular checks Opportunistic screening
Goals and actions: Dementia • Completion of a dementia pathway for early intervention including working age dementia to include:- • Primary care screening and identification • Assessment and personalised care plan undertaken by appointment of a specialist dementia nurse in primary care • Ongoing support with care coordinator linked to family and carer support • Specialist intervention via old age psychiatrist for anti-dementia medication • Psychology support • To implement a speech and language service for dementia patients • Dementia Strategy group in place to address National actions
What can you do? Screening, bloods, CT if vascular dementia suspected, and then refer. Watch this space!
Critical Success Factors • In summary: • Sign up to BUPA tool • Sign-up to the LESs – diabetes, COPD, AF, vascular checks • Remember opportunistic screening • Use community teams – neurology, heart failure, diabetes, stroke • Follow pathways, use evidence-based practice • Patient education and self-care • Give us feedback and ideas!