Download
1 / 15
150 likes | 333 Views
Developing a new public health intelligence system in the North West of England. Health Statistics Users Group 25 th March 2011 James Mechan Head of Public Health Intelligence. Drivers. PH White paper states that PH England;

E N D
Developing a new public health intelligence system in the North West of England Health Statistics Users Group 25th March 2011 James Mechan Head of Public Health Intelligence
Drivers PH White paper states that PH England; • ‘will continue working closely with the full range of public health partners involved in surveillance, monitoring, evaluation and intelligence in order to develop a clear approach for information and intelligence • ‘will work to eliminate gaps and overlaps and to develop the specialist workforce required’ • will bring together public health functions that are carried out in different parts of the system at present into a new, streamlined whole so as to remove duplication and drive efficiencies and innovation
Drivers Importantly it states that • ‘Public Health England offers a unique opportunity to draw together the existing complex information, intelligence and surveillance functions performed by multiple organisations into a more coherent form and to make evidence more easily available to those who will use it, in a form that makes it most likely to be used. • The White Paper also describes the role of public health evaluation and research as being critical in enabling public health practice to develop into the future and address key challenges and opportunities, such as how to handle the wider determinants of health and how to use behaviour change science to support better practice
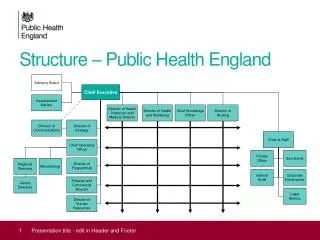
The Current System in the North West • Recent mapping exercise by LJMU (Nov 2010) suggests a total public health analytical capacity of 89.8 wte • 27.2 wte at regional / sub-regional level (incl. NWPHO) • 24.1 wte in Cheshire and Merseyside • 2.6 wte in Cumbria • 10.1 wte in Lancashire • 25.8 wte in Greater Manchester • Almost 50% reduction in total number of analysts between March and November 2010 – still reducing • Decrease particularly evident in posts at Grades 6 and 7 • Major reduction in analysts in training posts
Implications of structural changes (1) • Expanded customer base for public health intelligence that includes public health, the local authority, GP Consortia and other agencies represented on the HWBB • Strengthened role of JSNAs and the greater focus on these through the PCT cluster arrangements/GP Consortia increases the need for robust public health information, intelligence and analysis at a LOCAL level • The transfer of public health responsibilities to local authorities raises issues regarding the relationship between existing public health intelligence teams and the research and intelligence functions of local authorities
Implications of structural changes (2) • Growing ‘brokerage’ role for public health intelligence teams in reviewing the market to understand what is on offer, where it can enhance existing work and advising local authorities and GP Consortia of the quality of products available from ‘information intermediaries’ • Reductions in the availability of core data from national sources may mean that public health intelligence teams will have to produce more information themselves or purchase it from a commercial source • Diversion in focus between more centralised national public health intelligence system and local public health intelligence teams
Future Public Health Intelligence System: Core Principles • Subsidiarity: Intelligence work needs to take place as close as possible to the people and strategies that require it • Localism: Local intelligence professionals and partnerships are the building blocks for intelligence structures at supra-local level. • Partnership: System based on stronger, more formal, partnerships with existing intelligence providers rather than on a totally new layer of intelligence (e.g. a supra-local observatory) • Diversity: Different elements of the intelligence-base may be provided by a range of different suppliers rather than by a single organisation • Evidence-led: Work should only be done at supra-local level where it is clear that this work will benefit all partners or contribute to the development or expansion of an evidence base for that topic
The Challenge for Public Health Intelligence The PH White paper asks what are the best opportunities; • to develop and enhance the availability, accessibility and utility of public health information and intelligence • To address current gaps such as using the insights of behavioural science, tackling wider determinants of health, achieving cost effectiveness and tackling inequalities? • To ensure that wider partners nationally and locally contribute to improving the use of evidence in public health?
Greater Manchester Public Health Intelligence Transition Project • Aims to describe the different elements of the current public health intelligence system and articulate what the system might need to look like in the future in the context of the changing public health and NHS structures • Recommends moving towards a hub and spokes model of public health intelligence across GM by April 2012 • Future focus to include management, reporting and sharing of public health data; improved communication and coordination of intelligence activities; and developing the professional and non-professional workforce • Agreed by DsPH on 4th March 2011
Cheshire and Merseyside • Using Large Scale Approach to develop a new public health system across Cheshire and Merseyside • Identified public health intelligence and knowledge management as one of the priorities to review the functionality and develop a model to support commissioning • Task and Finish Group established and met in January to agree functionality and optimum delivery i.e. local, county, sub-regional etc • Option paper being drafted for consideration by Cheshire and Merseyside DsPH in March 2011
Intelligence for Healthy Lancashire Group • Proposal to pull together all the public health intelligence resources within the county into a single Lancashire Public Health Intelligence Unit (Intelligence for Healthy Lancashire Team from June 2011) • Initial stage to bring together public health intelligence staff from 3 Lancashire PCTs but to widen this to include county-wide analysts in the future (from 1st April 2012) • Primary focus likely to be on providing a range of core public health intelligence outputs • DsPH agreed proposals in principle in January 2011 • Links to an existing data repository facility for PH and NHS data
The contrast between local and national public health intelligence system needs
The contrast between local and national public health intelligence system needs
Acknowledgments • Neil Bendel - NHS Manchester/ Greater Manchester (GM) PH Intelligence Network • Paul Langton - Public Health Intelligence Manager, NHS Knowsley / Knowsley MBC • Mark Bellis - North West Public Health Observatory (NWPHO)