Download
1 / 26
430 likes | 1.89k Views
adejare i e. Outline . HydroceleIntroduction ClassificationClinical presentation and diagnosisComplicationsTreatment. adejare i e. Hydrocele. Introduction Collection of fluid in the tunica vaginalisA very common cause of scrotal swelling The diagnosis can often be made on physical examinat

E N D
1. adejare i e INTRASCROTAL PATHOLOGIES: Hydrocele, Testicular Torsion and Epididymo - Orchitis Dr Adejare I E
Senior Registrar
Urology Unit
Department of Surgery
OAUTHC
2. adejare i e Outline Hydrocele
Introduction
Classification
Clinical presentation and diagnosis
Complications
Treatment
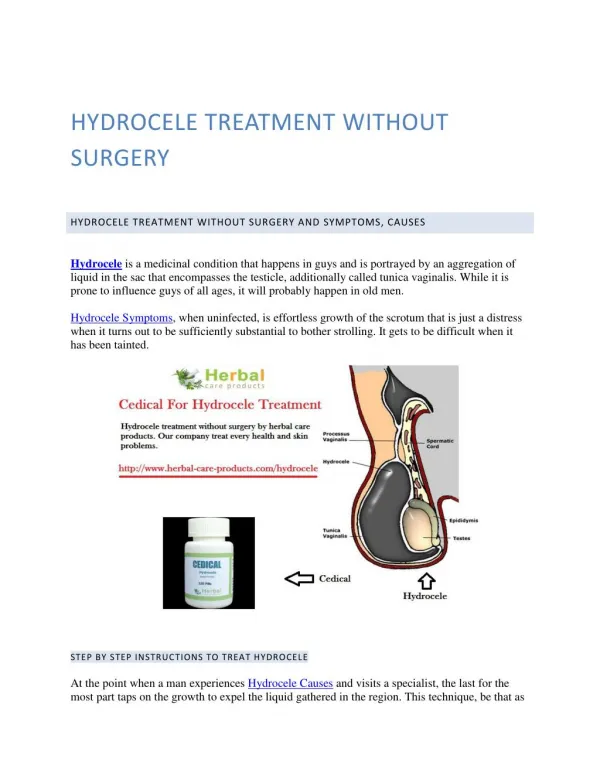
3. adejare i e Hydrocele Introduction
Collection of fluid in the tunica vaginalis
A very common cause of scrotal swelling
The diagnosis can often be made on physical examination alone
Tunica vaginalis is the remnant of the processus vaginalis
4. adejare i e Classification
Anatomic
Vaginal hydrocele
Hydrocele of the cord
Communicating hydrocele
Infantile hydrocele
Aetiologic
Congenital
Persistence of the processus vaginalis
Often seen in neonates, infants and childhood
Primary/ Idiopathic
Due to defective absorption of fluid
Secondary
Increased fluid production
Epididymo orchitis
Testicular tumour
Torsion
Trauma
Reduced absorption
Post hernoirraphy, varicocelectomy
filariasis
5. adejare i e
6. adejare i e Clinical presentation and diagnosis Depends on the anatomic / aetiological type
Vaginal
History
Most common in middle to late adulthood
Slow growing and painless
Present for many years before presentation
Features of its aetiology if secondary
Examination
Scrotal swelling (can get above the swelling)
No cough impulse
Testis palpable if lax, may not be palpable if tense
Transilluminates brilliantly
7. adejare i e Communicating hydrocele
neonate, young infant or child. May present in adolescence
History
Enlarges with increased intra abdominal pressure, change in position
Can be emptied
Examination
Soft/tense scrotal swelling,
Testis may or may not be palpable
Transilluminates brilliantly
Infantile hydrocele
Similar pathology to communicating hydrocele
Doesn�t empty
8. adejare i e Hydrocele of the cord
Mobile, smooth , oval
Moves downwards if the testis is pulled downwards
Differential
Inguinal hernia, lipoma of the cord
Investigations
Scrotal ultrasound
If the diagnosis is not clear
Testis is not palpable
Secondary hydrocele is suspected
9. adejare i e Complications
Infection
haematocele
10. adejare i e Treatment Surgery
Communicating hydrocele/ hydrocele of the cord
Groin incision
High ligation of the patent processus vaginalis
Vaginal
Trans scrotal approach
Hydrocelectomy
Lord�s
Jaboulay�s
11. adejare i e Intra operative photograph : Vaginal Hydrocele
12. adejare i e Non operative
Communicating hydrocele before 12 � 18 mo of age
Elderly patients who cannot tolerate anaesthesia
Drainage with a cannula
Injection of sclerosant
13. adejare i e Testicular torsion Introduction
Twist of the cord with subsequent ischaemia
May lead to loss of the testis
Classification
Intravaginal torsion
Cord twists within the tunica vaginalis
Occurs in adolescents and adults
Extravaginal torsion
Cord twists outside of the tunica vaginalis
Occurs in neonates/ prenatal
14. adejare i e Pathology/ Aetiology
Cord twists on itself
May be up to 720 degrees
Predispositions
High investment of tunica vaginalis
Horizontal lie
Long mesoorchium
Undescended testis
15. adejare i e Pathogenesis Twist of the cord
Venous and arterial occlusion
Anaerobic respiration with hypercarbia, hypoxia and acidosis
Ischaemic pain
Oedema and haemorrhage set in
Irreversible ischaemic injury by 4 hours
Degree of twisting determines the salvagability of the testis
Reduction of the twist leads to ischaemic reperfusion injury
16. adejare i e Clinical features Intravaginal
Pubertal males
Most occur during sleep
May be precipitated by trauma/ athletic activity
Testicular pain
Sudden onset
Nausea and vomiting
Pain referred to the ipsilateral lower abdominal quadrant
Usually no urinary symptoms or fever
17. adejare i e High riding testis in a right testicular torsion
18. adejare i e Examination
High riding testis with foreshortened cord
Abnormal testicular lie
Swelling
Absent cremasteric reflex
Pain increased on elevating the testis
Investigation
A clinical diagnosis
Doppler ultrasound
Radionuclide imaging
When in doubt, explore
19. adejare i e Treatment
Scrotal exploration
EXPLORE AND FIX BOTH TSETIS
Marginal viability
Warm sponge
100% oxygen
Remove necrotic testis
20. adejare i e Necrotic testis
21. adejare i e Epididymo orchitis Inflammation of the epididymis and testis
May be acute or chronic
testis
22. adejare i e Pathogenesis/ Aetiology
Retrograde
From the urinary tract via the ejaculatory ducts and vas
Starts at the tail of the epididymis and spreads to the rest of the organ and the testis
Young boys/ infants
UTI/ genitourinary congenital anomaly
Uncircumcised
Elderly men
LUTO from BPH, CAP
Catheterisation + associated infection
Sexually active men < 35 years
Usually secondary to sexually transmitted infections
Adult males
Secondary prostatitis
23. adejare i e Chronic prostatitis
Result from
Inadequately treated acute epididymitis
Recurrent epididymitis
Tuberculosis and other chronic granulomatous infections
Bacteriology
Paediatric/ Elderly patients
Coliforms
Sexually active men
Heterosexual
Gonococcus and Chlamydia
Homosexual
E. Coli and H. Influenzae
24. adejare i e Diagnosis History
Recent onset testicular pain
Lower quadrant abdominal discomfort
Nausea/ Vomiting
Dysuria, urethral discharge
Examination
Swollen tender epididymis and testis
Prehn�s sign
Fever
Urethral discharge
Tender prostate
25. adejare i e Investigation Urethral swab/ smear for mcs
Urine for m/c/s
Doppler USS
Infants/ Elderly patients
Imaging
Abdominal/ Pelvic ultrasound
Cystourethrography
IVU
Urethrocystoscopy
26. adejare i e Treatment 4 � 6 week trial of antibiotics
Elevation of the scrotum/ scrotal support
Analgesia, antibiotics
Scrotal exploration if in doubt