Download
1 / 55
700 likes | 2.03k Views
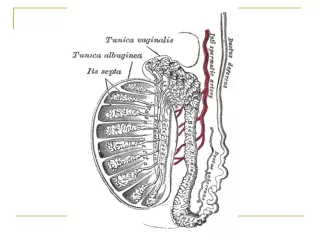
Testicular tumors. Mostafa El- Haddad. Anatomie. Blood Supply? Lns distribution: Cross over from Rt to Lt but not from Lt. to Rt. Scrotal Lymphatic's disruption. Epidemiology. Age: 20-35ys. Seminoma patient is older. Don’t forget that yolk sac tumor can occur in children. Where?

E N D
Testicular tumors Mostafa El- Haddad
Anatomie • Blood Supply? • Lns distribution: • Cross over from Rt to Lt but not from Lt. to Rt. • Scrotal Lymphatic's disruption.
Epidemiology • Age: 20-35ys. • Seminoma patient is older. • Don’t forget that yolk sac tumor can occur in children. • Where? • Social problem.
Etiology and Risk Factors • Intrauterine exposure to Estrogen. • Un-descended testis: intra-abdminal > inguinal. • Family history : very important. • AIDS: RPL and stage is difficult to predict. Stage for stage is ok. Or c h id o p e x y d o e s n o t r e d u c e r i s k i n al l a g e g r o u ps b u t f a c i l i t a t e s e x a m i n a t i o
Intratubular neoplasm? How we detected? • Present in the contralateral testis in 10%. • Bilateral testicular tumor do exist.
Pathology • Germ Cell tumors. • Supporting Cell tumors. • Lymphoma. • Metastasis including sanctuary site.
WHO ClassificationAndBritish Testicular Tumor Panel and Registry
Isochromosome 12 • What is isochromosome? • Value? • Pathognomonic feature of GCT of all histologic types, whether of gonadal or extragonadal origin. • Can be an early marker (reported in insitu tumors). • The presence of three or more copies of i(12p) has been correlated with poor prognosis GCT.
Natural History • Seminoma associated with more ureteric obstruction? • NSGCT is more aggressive go blood.
Other Lymph Nodes • External Iliacs • Obturator. • Inguinal .
SpermatocyticSeminoma • Sixth decade. • Bilateral more. • Indolent course. • Treatment surgery. • -ve PLAB
Intratubular Germ cell Neoplasia • Precursor but not for SS: • Found in high risk group. • Found adjacent to cancer. • 50% risk to transform at 5 years. • 100% risk at 8 years. • Treatment : Radiotherapy 18 to 20Gy.
Symptoms and Signs • Pain: local, Back. • Gynecomastia? • DD: testicular torsion, hydrocele, varicocele, spermatocele, and epididymitis
Orchiectomy may occasionally be delayed in metastatic cases to control primary disease . • Orchiectomy should be done? • When orchiectomy should not be done?
HCG • HCG: alpha unit and beta unit. • prostate, bladder, ureteral, and renal cancers may show increase in B-HCG elevation. • Spurious elevations have been noted in persons using marijuana. • Cis-platinum-induced testicular atrophy in the remaining testis, resulting in lower levels of testosterone, with a compensatory hypersecretion of LH to stimulate Leydig cell secretion of testosterone.
To Make Life More Complicated • Neuroendocrine tumors and cancers of the bladder, kidney, lung, head and neck, GI tract • Specifically gastric, pancreatic, biliary, and colorectal cancers, cervix, uterus, and vulva.
In addition, there are case reports of elevations in hCG in lymphoma and leukemia.
HCG produced by Scincytiotrophoblast. • Seminoma can produce HCG 5-40% of cases. • Not more than 100 IU.
AFP • Pregnant women (Hamel). • Hepatitis. • Hepatocellular carcinoma. 3 H
LDH • Gene that encodes LDH isoenzyme 1 maps to chromosome 12. • The serum level of LDH isoenzyme 1 has been shown to correlate with the number of copies of i(12p) in the tumor, a fairly specific genetic marker of germ cell malignancies. • Furthermore, the presence of three or more copies of i(12p) has been correlated with a worse prognosis.
Very Important • Up to 30% of patients with early-stage non-seminomatous GCT will have normal serum markers, so the absence of marker elevation should not influence the decision to perform an orchiectomy. • Eventhough markers should be done before and After Surgery.
PET-CT • FDG-PET was unable to detect mature teratomas as well as lesions smaller than 5 mm in diameter. Not routinely used or recommended in initial staging. • Can be used to differentiate between residual disease and fibrotic bands?
Other Investigations • Brain imaging in Choriocarcinoma. • In patients with clear clinical examination and Elevated markers don’t forget to investigate the other testis.
Stage I Seminoma • Orchiectomy PLUS 1- Observation When? Or 2- Radiotherapy When? Or 3- Chemotherapy What?
Chemotherapy in advanced Stage • BEP or EP • Cisplatin is better than Carboplatin
Spermatic cord involvement necessitates a radiation field that covers the entire inguinal orchiectomy scar, whereas scrotal skin involvement mandates radiation to the hemiscrotum
Residual Disease Post Chemo • Less than 3 cm or more than 3cm. • Post chemotherapy field of radiation??
Consent. • Preparation. • Positioning. • Simulator. • 30 degrees rotation of the remaining testis from the patient’s long axises.
TesticualtIrrdiation • Intratubular germ cell tumor. • Testicular leukemia or lymphoma. • Position is the Key. • Penis. • Beam arrangement. • Energy: deep X- Electron, Photon. • Bolus Where???
Technical consideration • Adjuvant radiotherapy to the hemiscrotum and ipsilateral inguinal lymph nodes is recom- mended. • The scrotal field is matched to the tattoo at the inferior border of the dog-leg field.
Non Seminoma • Vascular/lymphatic invasion • Embryonal carcinoma elements (>30%) • Absence of yolk sac elements • Absence of AFP preorchiectomy • Less than 50% teratoma • Local extension into paratesticular structures