Download
1 / 46
460 likes | 528 Views
This module covers caring for children with neurosensory alterations, neurological assessment techniques, cranial nerve functions, and detecting signs of increased intracranial pressure. It also addresses neuromuscular signs, diagnostic procedures, and common cerebral trauma issues. Watch videos for a hands-on understanding and learn about meningitis, its causes, symptoms, and diagnostic and treatment procedures.

E N D
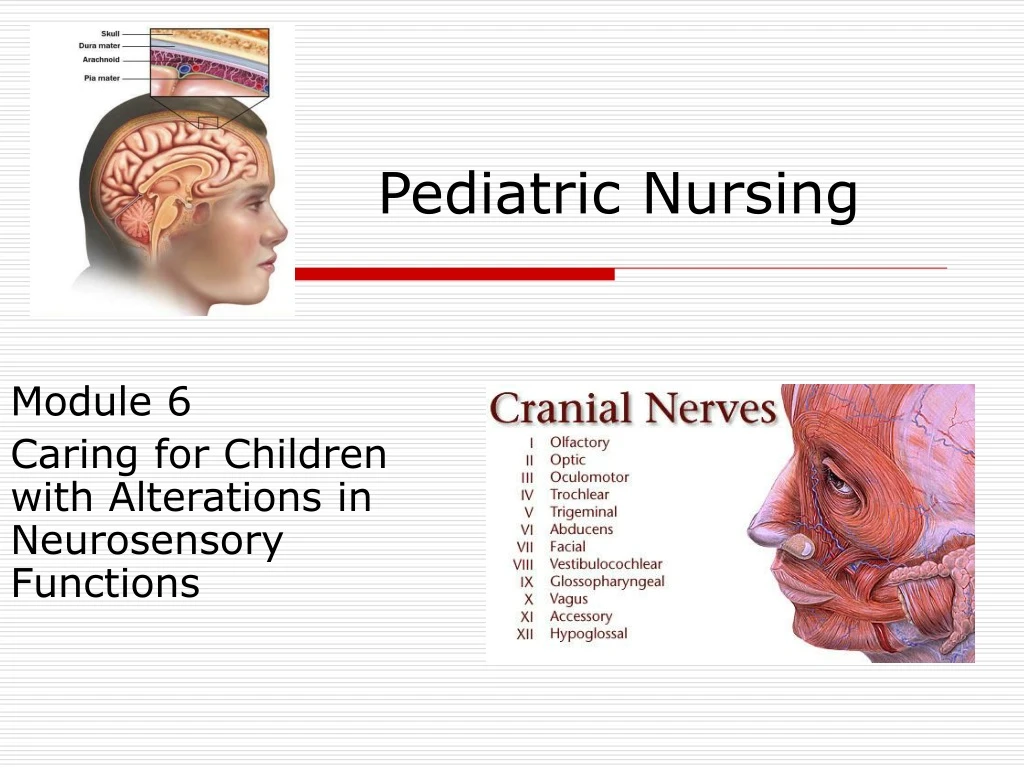
Pediatric Nursing Module 6 Caring for Children with Alterations in Neurosensory Functions
Neurological Assessment • Assessment • indirect measurements • children under 2 years • normal growth and development parameters • parents evaluation of their child • developmental milestones • history • prenatal • birth history • post natal
Neurological Assessment • Behavior • personality, affect, level of activity, social interaction, attention span • Motor function • muscle - size, tone, strength • abnormal movements • Sensory function • discrimination of touch with eyes closed
Neurological Assessment • Cranial Nerves • Olfactory - smell • Optic - light perception visual acuity • peripheral vision • Ocular motor - 6 cardinal positions of gaze PERRLA • Trochlear - have child look down and in • Trigeminal nerves - bite down and try to • open jaw, sensation to face
Neurological Assessment • Abducens- look toward temporal side • Facial - make a funny face or smile • Acoustic - hearing and balance • Glossopharyngeal - gag reflex, taste • Vagus - uvula is midline, swallow • Accessory - shrug shoulders against mild applied pressure • Hypoglossal - move tongue in all directions
http://video.google.com/googleplayer.swf?docid=3314499774483652601&hl=en&fs=truehttp://video.google.com/googleplayer.swf?docid=3314499774483652601&hl=en&fs=true Video - Neurological exam in children http://video.google.com/googleplayer.swf?docid=7363212422012619904&hl=en&fs=true http://video.google.com/googleplayer.swf?docid=-728577715202828264&hl=en&fs=true
Increased Intracranial Pressure • Causes • tumors • accumulation of fluid within the ventricular system • bleeding • edema in cerebral tissues • early signs and symptoms are often subtle and assume many patterns
Assess for signs of Increased Intracranial Pressure • Level of consciousness (LOC) • earliest indicator of changes in neurological status 1. Alertness • arousal-waking state • ability to respond to stimuli 2. Cognitive abilities • process stimuli • produce verbal and motor responses
Increased Intracranial PressureSigns/symptoms • Lack of painful stimuli is abnormal and is reported immediately • as ICP increases LOC decreases • 3. Vital Signs • pulse • variable, may be rapid or slow, bounding or feeble • B/P • normal or elevated with a widening pulse pressure, at shock level • Respiration's • varies
Increased Intracranial PressureSigns/symptoms • Temperature • elevated especially with infections and intracranial bleeding • subnormal in a coma of toxic origin • Pupils • size and reactivity • bilateral vs unilateral • sudden fixed and dilated pupils is a neurosurgical emergency • pressure from herniation of the brain through the tentorium
Neuromuscular - Signs/symptoms • Neuromuscular Movement • strength, spontaneous movements • asymmetric or absent movements • tone • may be increased or decreased • tremors, twitching, spasms • purposeless flapping • hyperactive or flaccid
Increased Intracranial Pressure Signs/symptoms • Posturing • decorticate • adduction and flexion • decerebrate • rigid extension and pronation
Diagnosis Procedures • Lumbar puncture • measure pressure and sample for analysis • Subdural tap • r/o subdural effusions, relieves ICP • EEG • measures electoral activity • detects abnormalities
Diagnosis Procedures • Computer Tomography (CT) • visualizes horizontal and vertical cross section of the brain • distinguishes density • MRI • permits tissue discrimination unavailable with other techniques • Transillumination • localized glowing seen in abnormal fluid
Diagnosis Procedures • Labs • CSF • blood glucose • electrolytes • Ca, Mg, Na • clotting studies • liver function tests • blood cultures • drug titre
Cerebral TraumaHead Injury • Etiology • falls, MVA, bicycle injuries • head is larger, heavier • children curious • incomplete motor development • Concussion • Contusion/laceration • Fracture
Shaken Baby Syndrome coup countrecoup
Fatal bacterial meningitis
Meningitis • Inflammation of the meninges • Spread • vascular dissemination • OM or URTI • exudate covers the brain • brain becomes hyperemic and edematous
Meningitis • Causative Organism • H. Influenza, type B • S. Pneumoniea • N. Meningitis • Meningococcus • Signs and Symptoms • FUO • lethargy
MeningitisSigns/symptoms • irritable • vomiting and/or diarrhea • signs of meningeal irritation • guarding of the neck • nuchal rigidity • cries when moved • poor feeding
MeningitisDiagnosis • Labs • CSF • culture, glucose, protein, cell count, gram stain • Blood Culture • r/o sepsis • Urine Culture • r/o UTI • Chemistry panel • electrolytes, glucose, BUN, creatinine
MeningitisTreatment • Antibiotics • administer within 1 hour of diagnosis • type is based on age and causative organism • neonate - ampicillin / claforan • 3 months to 3 years - ampicillin / ceftriaxone • older children - penicillin / chloramphemicol
MeningitisTreatment • Fluid Management • fine balance between dehydration and cerebral edema • child may be dehydrated due to v/d, poor po, fever • 2/3 maintenance of IV replacement • fluid restriction
MeningitisNursing Care • PC: Neurological dysfunction • cerebral hypoxia • seizures • increased ICP • PC: Seizure • High Risk for spread of infection • needs resp. isolation for first 24 hrs of antibiotic therapy
MeningitisNursing Care • Fluid Volume Deficit: less than body requirements r/t dehydration • NPO/fluid restriction • I & O • daily weights • Labs • specific gravity and electrolytes • IV fluid - careful, conservative replacement
MeningitisNursing Care • PC: Neurological damage • seizures • sequelae to meningitis • seizures • hydrocephalus • visual/hearing deficits
Reye Syndrome • Toxic encephalopathy with additional organ involvement • Etiology • follows viral illness, ASA • Signs and Symptoms • fever • decrease LOC • hepatic dysfunction • Prognosis • good
Febrile Convulsions • Age • most common between 6 months and 3 years • Occurrence • Seizure accompanied by fever without CNS infection • Occurs during the temperature rise • Treatment • fever - tylenol • seizure - ativan, valium
Tonic clonic seizure • Tonic – stiff • Clonic - jerking • Rescue position
Assessment • seizure precautions • emergency treatment • rescue position • Nursing Care • protect from injury • open airway • accurately observe and record happenings
Hydrocephaly • Abnormal condition characterized by an increase volume of normal cerebrospinal fluid under increased pressure with in the intracranial cavity • Communicating • obstruction is located in the subaranoid cistern or within the subarachnoid space • Non-communicating • blockage is within the ventricles
Hydrocephaly - Pathology • 3 possible mechanisms leading to hydocephalus • 1. Over production of CSF • 2. Defective absorption of CSF • 3. Obstruction of CSF • 3 major causes • inflammation • congenital malformations • tumors
HydrocephalusSigns/symptoms • Signs of increased fluid pressure • tense or bulging anterior fontanel • scalp becomes thin and shiny • vein dilate • cranial suture lines begin to separate • Other clinical symptoms • vomiting • wide bridge between eyes • bulging eyes - sunset eyes
HydrocephalusSigns/symptoms • Severe Form • head size increases rapidly • infant’s cry is shrill, high pitched • hyperirritability, restlessness • Older Children • no head enlargement ataxia • papilledema Alter mental status • spasticity strabismus • H/A
HydrocephalusTreatment • Surgical • VP (ventriculo-peritoneal) Shunt • Nursing Care • Pre-op • assessments • daily head circumference • size and fullness of anterior fontanel • behavior • nutrition - vomiting
Hydrocephalus - Nursing Care • fluid and electrolyte needs • positioning • prevent pressure ulcers • support the neck • good skin care • neuro assessments • LOC • irritable child/infant • vital signs • observe for seizures
Hydrocephalus • Nursing Care • Post-op • monitor feeding and behavior patterns • assess for increasing ICP and cerebral irritability • HOB flat or set elevation • Shunt observation • infection - along the line or cerebral • abdominal girth • valve function, blockage, separation • emotional needs - hold and cuddle • teaching
Cerebral Palsy • Non-specific disorder characterized by early onset of movement and posture impairments • abnormal muscle tone and coordination • Spastic • hypertonicity, stiff • Dyskinectic • slow, worm-likemovement
Spina bifia - myelomeningocele • Failure of the neural tube to close during early development • Treatment • early surgical closure • Associated Problems • hydrocephalus • paralysis • bone deformity
Andrew, age 10 was a passenger in a MVA 3 weeks ago, he sustained a closed head injury from the impact. He is unconscious in the E.R. • What are is needs in the Emergency Room? • What are his priority nursing interventions?
He was admitted to the PICU, now transferred to your Pediatric Unit. He tracks his parents movement, he is receiving 02 via trach collar, has G-tube with enteral feedings, is incontinent of urine and stool, is able to nod his head appropriately. • Why do you think Andrew has a trach? • Why do you think Andrew has a G-tube?
What risk factors predispose Andrew to infection? • Why is he on these medications? • ranitidine 70mg bid - zantac • metoclopramide 3.5 mg qid - reglan • phenytoin sodium 70mg bid - dilantin • How can you intervene to help met Andrew’s growth and development needs?