Download
1 / 15
170 likes | 850 Views
Migraine Prophylaxis in Patients with Patent Foramen Ovale:. PFO Closure vs. Traditional Preventative Measures By: Samantha Howell Submitted to: Dr. Gurwell. Migraines. 28 million Americans each year

E N D
Migraine Prophylaxis in Patients with Patent Foramen Ovale: PFO Closure vs. Traditional Preventative Measures By: Samantha Howell Submitted to: Dr. Gurwell
Migraines • 28 million Americans each year • Characterized by: pulsing or throbbing pain, unilateral pain commonly, interferes with daily activities, worsened by physical activity • Has to be accompanied by one of the following: N/V, photophobia, or phonophobia • 2 types: Migraine with aura (20%) Migraine without aura (80%) • Aura-a sensory disturbance (visual typical)
Pathophysiology • Poorly understood • Excitation wave theory • Cerebral ischemia • Lungs may play a role -if bypassed allow microemboli and substances like serotonin and ADP to get to the brain via circulation -one possibility is PFO or ASD Neurovascular cause
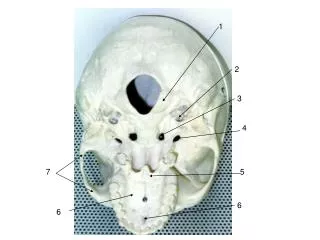
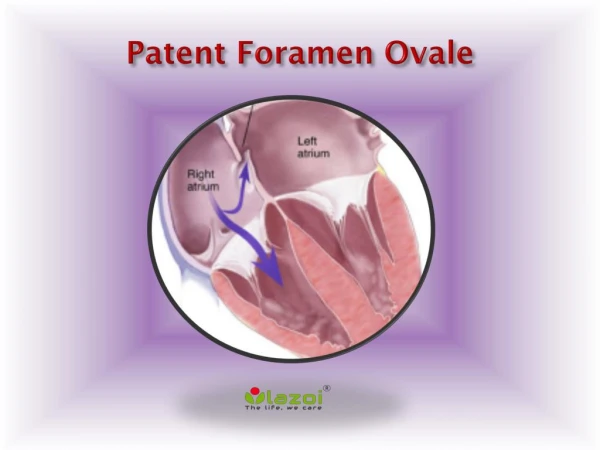
Patent Foramen Ovale • Failure of foramen ovale to close at birth • Right-to-left shunt of blood • PFO may be present in 40-60% of migraine with aura sufferers • Closing this defect may be a future treatment for migraine
Traditional Migraine Prophylaxis • Avoidance of Triggers • Stress Management • Pharmacological Prophylactic Treatments used if MHA occurs more than 2x a month, not controlled with acute tx, or the patient takes abortive tx more than 2x a week • Anti-epileptics (Topiramate, Gabapentin) • NSAIDS (Ibuprofen) • Antidepressants • Beta blockers (Atenolol) • Calcium channel blockers (Verapamil) • ACEi (Lisinopril) • Magnesium • Botox • Other Vitamins/Minerals
Clinical Question • In patients with migraine with aura who have a known patent foramen ovale (PFO), is there a quality-of-life benefit to PFO closure surgery or would migraine symptoms be equally controlled with pharmacological prophylactic treatment? • Methods: Three PubMed Database searches were performed to attempt to answer this question
Wilmshurst, 2000 • Retrospective study looking at effects of PFO closure on migraine headaches (n=21) • Surgery was performed to treat decompression illness • Treated with aspirin for 6 mos. post-op • Patients were interviewed about migraine after the surgery (had to recall symptoms before and after procedure)-IHS guidelines used to determine if patients had migraines • 9-32 month follow-up
Giardini, 2006 • Prospective study looking at long-term efficacy of PFO closure on migraine in stroke patients (n=13) • Surgery was performed due to previous stroke • Treated with aspirin for 12 months following the surgery • Patients were interviewed about migraine and the condition severity was assessed using MIDAS questionnaire • 4.9 ± 1.4 years follow-up
Results Table 1-Effect of PFO closure on migraine headaches
Silberstein, 2004 • Randomized, double-blind, placebo-controlled trial (n=284) • 26 week treatment period using 50, 100, or 200 mg/d of Topiramate and matching amounts of placebo • Patients kept diaries recording periods with migraine headache • Success of the drug was based on change from baseline • Percentage of patients with decreased frequency and severity in each group: 100 mg/d Topiramate = 54% 200 mg/d Top. = 52.3% 50 mg/d Top. = 35.9% Placebo = 22.6%
Schrader, 2001 • Randomized, placebo controlled, crossover study (n=60) • 30 pts. took 10 mg Lisinopril once daily for 1 wk and then two 10 mg tablets once daily for 11 wks followed by 2 wk washout period-then one placebo pill daily for one wk and then two placebo pills once daily for 11 wks. • Another 30 pts. took the placebo pills during the first 12 wks and lisinopril during the next 12 wks • Patients also recorded symptoms in a diary • Results: -For days with migraine, a reduction by at least 50% was seen in 30% of participants -32% of participants saw at least a 50% reduction in headache severity compared to placebo period
For Comparison Table 2-Reduction of migraine activity by PFO closure vs. Traditional Migraine Prophylaxis
Study Strengths and Limitations • Limitations (PFO) • Sample size • Retrospective (Wilmshurst, 2000) • Participant Recall error • Limitations (All) • All data gathered was somewhat subjective (participant diaries, etc.) Strengths (PFO) • MIDAS • IHS • Follow-up 5 yrs Strengths (Meds) • Randomized, placebo-controlled • Large number of subjects • Quantitative measures
Conclusions • PFO closure looks promising-higher percentage of patients in the PFO closure trials had reduced frequency and severity of migraines • PFO closure is invasive and there is not enough research • Additionally, not everyone who has migraines has the heart wall defect • The surgical procedure should only be recommended at this time for individuals with multiple conditions related to PFO • Our patients with PFO and migraines should simply be placed on traditional prophylactic meds or use acute treatment until more research is done
References • Beda RD, Gill Jr. EA. Patent foramen ovale: does it play a role in the pathophysiology of migraine headache? Cardiol Clin. 2005;23:91-96. • Buchanan TM, Ramadan NM. Prophylactic pharmacotherapy for migraine headaches. Semin Neurol. 2006;26:188-198. • Giardini A, Donti A, Formigari R, Salomone L, Palareti G, Guidetti D, et al. Long-term efficacy of transcatheter patent foramen ovale closure on migraine headache with aura and recurrent stroke. Catheter Cardiovasc Interv. 2006;67:625-629. • Headache Classification Subcommittee of the International Headache Society. The international classification of headache disorders, 2nd edition. Cephalalgia. 2004;24(Suppl. 1):1-36. • Lipton RB, Scher AI, Kolodner K, et al. Migraine in the United States. Neurology 2002;58:885. • Lipton RB, Stewart WF, Sawyer J, Edmeads JG. Clinical utility of an instrument assessing migraine disability: The migraine assessment (MIDAS) questionnaire. Headache 2001;41:854-861. • Modi S, Lowder DM. Medications for migraine prophylaxis. Am Fam Physician. 2006 Jan 1;73(1):72-78. • Morandi E, Anzola GP, Angeli S, Melzi G, Onorato E. Transcatheter closure of patent foramen ovale: a new migraine treatment? Journal of Interv. Cardiol. 2003;16(1):39-42. • Parsekyan D. Migraine prophylaxis in adult patients. West J Med. 2000;173:341-345. • Schrader H, Stovner LJ, Helde G, Sand T, Bovim G. Prophylactic treatment of migraine with angiotensin converting enzyme inhibitor (lisinopril): randomized, placebo controlled, crossover study. BMJ 2001;322:1-5. • Schwedt TJ, Dodick DW. Patent foramen ovale and migraine-bringing closure to the subject. Headache. 2006:46:663-671. • Schwerzmann M, Nedeltchev K, Meier B. Patent foramen ovale closure: a new therapy for migraine. Catheter Cardiovasc Interv. 2007;69:277-284. • Silberstein S, Neto W, Schmitt J, Jacobs D. Topiramate in migraine prevention. Arch Neurol. 2004;61:490-495. • Silberstein SD, Goadsby PJ. Migraine: preventative treatment. Cephalalgia 2002;22(7)491-512. • Wilmshurst P, Nightingale S, Pearson M, Morrison L, Walsh KP. Relation of atrial shunts to migraine in patients with ischemic stroke and peripheral emboli. Am J Cardiol. 2006;98(6):831-833. • Wilmshurst PT, Nightingale S, Walsh KP, and Morrison WL. Clopidogrel reduces migraine with aura after transcatheter closure of persistent foramen ovale and atrial septal defects. Heart. 2005;91(9): 1173-1175. • Wilmshurst PT, Pearson MJ, Nightingale S, Walsh KP, Morrison WL. Inheritance of persistent foramen ovale and atrial septal defects and the relation to familial migraine with aura. Heart. 2004; 90(11):1315-1320. • Wilmshurst PT, Nightingale S, Walsh KP, Morrison WL. Effect on migraine of closure of cardiac right-to-left shunts to prevent recurrence of decompression illness or stroke or for haemodynamic reasons. Lancet. 2000; 356(9242):1648-1651.