Download
1 / 26
440 likes | 2.67k Views
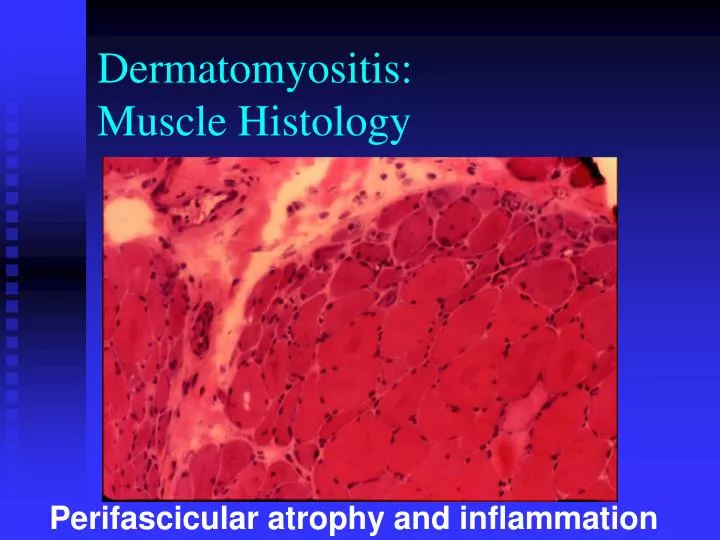
Dermatomyositis: Muscle Histology. Perifascicular atrophy and inflammation. Dermatomyositis Muscle Histology. Perifascicular atrophy. Vascular Hypothesis: Complement-mediated microangiopathy Deposition of complement (MAC) and antibody Reduced muscle capillaries Ischemic damage to muscle

E N D
Dermatomyositis:Muscle Histology Perifascicular atrophy and inflammation
Dermatomyositis Muscle Histology Perifascicular atrophy
Vascular Hypothesis: Complement-mediated microangiopathy Deposition of complement (MAC) and antibody Reduced muscle capillaries Ischemic damage to muscle Nailfold capillary changes Cutaneous ulcerations Intestinal perforation Pathogenesis of Dermatomyositis
Histopathology of DMDalakas: Rheum Dis Clin 28:779,2002 Normal capillaries Reduced, abnormal capillaries
Nailfold Changes Figure from American College of Rheumatology slide collection
Nailfold Capillary Changes Normal Sclero-derma Adult DM JDM Narrow, straight, regular capillaries are normally seen. In scleroderma and DM, there is dilation, distortion, loss. (Figure and slide note caption from American College of Rheumatology slide collection)
Interferon Hypothesis type 1 interferons (α,ß) cause capillary, muscle fiber, and skin injury Interferon-producing cells in muscle Increase in type 1-interferon inducible proteins and mRNA transcripts in muscle Tubuloreticular inclusions in muscle capillaries Pathogenesis of Dermatomyositis
Histologic Patterns Dermatomyositis:Perifascicular Atrophy Polymyositis: Endomysial Infiltration
Gottron’s papules over fingers Gottron’s sign over extensor surfaces Heliotrope sign Erythematous rash Poikiloderma Photosensitivity Nailfold changes Mechanic’s hands Calcinosis Cutaneous ulcerations Cutaneous Features of Dermatomyositis
Dermatomyositis: Gottron’s Figure and caption from American College of Rheumatology slide collection
Dermatomyositis: Gottron’s See slide note for caption. Figure and caption from American College of Rheumatology slide collection
Dermatomyositis: Heliotrope Figure and caption from American College of Rheumatology slide collection
Dermatomyositis: Rash Figure and caption from American College of Rheumatology slide collection
“Mechanic’s Hands” From Miller FW. Myositis-specific autoantibodies: touchstones for understanding the inflammatory myopathies. JAMA 1993;270:1846-1849. See slide note for caption. Figure and caption from American College of Rheumatology slide collection.
Dermatomyositis: Calcinosis See slide note for caption. Figure and caption from American College of Rheumatology slide collection.
Additional Diagnostic Considerations • Magnetic Resonance Imaging and Spectroscopy • Autoantibodies (ANA, Specific autoantibodies) • Evidence of inflammatory/rheumatic disease (Fever, ESR, Arthritis, Raynaud's, ILD, vascular disease)
MAGNETIC RESONANCE IMAGING PM and DM • Can detect inflammation when biopsy, enzymes, and/or EMG are normal. • Can be used for: • Establishing diagnosis • Excluding myositis • Assessing inflammatory activity • Persistent weakness • Persistent enzyme elevation • Can identify site of active inflammation to direct biopsy
MAGNETIC RESONANCE IMAGING in IIM • Active disease best shown by T2-weighted images, reflecting increased water/edema. • Fatty replacement and atrophy also seen • Thighs most often studied • May be focal • Changes with disease activity
Dermatomyositis: Thigh (MRI) Figure and caption from American College of Rheumatology slide collection