Download
1 / 67
790 likes | 1.13k Views
Patella Fractures & Extensor Mechanism Injuries. Lisa K. Cannada, MD Revised: October 2008; May 2011. Anatomy. • Largest sesamoid bone • Thick articular cartilage proximally • Articular surface divided into medial and lateral facets by longitudinal ridge • Distal pole

E N D
Patella Fractures & Extensor Mechanism Injuries Lisa K. Cannada, MD Revised: October 2008; May 2011
Anatomy • Largest sesamoid bone • Thick articular cartilage proximally • Articular surface divided into medial and lateral facets by longitudinal ridge • Distal pole nonarticular
Anatomy • Patellar Retinaculum – Longitudinal tendinous fibers – Patellofemoral ligaments • Blood Supply – Primarily derived from geniculate arteries
Biomechanics • The patella undergoes approximately 7 cm of translation from full flexion to extension • Only 13-38% of the patellar surface is in contact with the femur throughout its range of motion
Biomechanics • The patella increases the moment arm about the knee – Contributes up to 30% improvement in lever arm • Patella withstands compressive forces greater than 7X body weight with squatting
Biomechanics • 2 X Torque: – Extend final 15° – Than to extend from a fully flexed position to 15 degrees of flexion
Physical Examination • Pain, swelling, contusions, lacerations and/or abrasions at the site of injury – Can determine timing of operative intervention • Palpable defect • Assessment of ability to extend the knee – Cannot perform a straight leg raise with no extensor lag
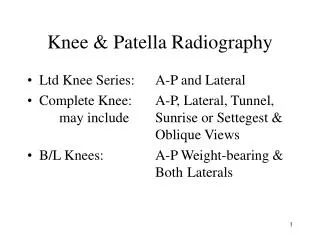
Radiographic Evaluation • AP & Lateral – Note patella height (baja or alta) – Note fracture pattern • Articular step-off, diastasis • Marginal impaction • Special views – Axial or sunrise • CT Scan - Occult Fractures - Complex or Marginal Impaction Fractures
Radiographic Evaluation • Bipartite Patella: • Don’t get fooled! – Obtain bilateral views – Often superolateral corner (Saupe Classification, 1923) – Accessory ossification center – Occurs 1-2% of patients
Etiology • Direct trauma – Direct blow to flexed knee (dashboard) – Increasing cases with penetrating trauma – Comminution & articular marginal impaction • Indirect trauma – Flexion force directed through the extensor mechanism against a contracted quadriceps – Simple, transverse fracture
Classification • Allows guidance with treatment • Types – Transverse – Marginal – Vertical – Comminuted – Osteochondral – Avulsion (not pictured) Tip: Vertical fractures may not result in disruption of extensor mechanism
OA/OTA Classification
Nonoperative Treatment • Indicated for minimally or nondisplaced fractures – < 2mm of articular step-off & < 3mm of diastasis with an intact extensor mechanism (extensor retinaculum) – If difficulty assessing, consider intra-articular injection of local anesthetic to better assess ability to extend • Consider for minimally displaced fractures in low demand patients (evaluate comorbidities & function) • Patients with a extensive medical comorbidities
Nonoperative Treatment • Long leg cylinder cast for 4-6 weeks – May consider a knee immobilizer or hinged knee brace for the elderly/low demand • Immediate weight-bearing as tolerated • Rehabilitation includes range of motion exercises with gradual quadriceps strengthening • Protect eccentric contraction 3 months
Operative Treatment • Goals – Preserve extensor function – Restore articular congruency • Preoperative Setup – Tourniquet (debatable) • Prior to inflation, gently flex the knee • Approach – Longitudinal midline incision recommended – Transverse approach alternative (dotted lines) – potentially higher risk wound problems, can limit initiation of ROM – Consider future surgeries!
Procedure Longitudinal Incision Clean Fracture Site Torn Retinaculum
Procedure Reduce & Compress Fracture
Operative Techniques • K-wires w/ tension band wiring (TBW) • Lag-screw fixation • Cannulated lag-screw with TBW (tension band screw – TBS) • Partial patellectomy • Total Patellectomy
Tension Band Wiring • Transverse, non-comminuted fractures • Reduce and clamp, then place two parallel 1.6mm K- wires placed perpendicular to the fracture • 18 gauge wire passed behind proximally and distally • Double Figure-8 wire for equal compression
Tension Band Wiring • Wire converts anterior distractive forces to compressive forces at the articular surface • Two twists are placed on opposite sides of the wire – Tighten simultaneously to achieve symmetric tension • Retinacular Injury – Keep open until the end – Window to assess articular reduction – Repair the retinacular injury last
Lag-Screw Fixation • Indicated for stabilization of comminuted fragments in conjunction w/ cerclage wires if necessary • May also be used as an alternative/adjunct to TBW for transverse or vertical fractures
Lag-Screw Fixation • Contraindicated for extensive comminution and osteopenic bone • Small secondary fractures may be stabilized with 2.0mm, 2.7mm or 3.5mm cortical screws • Reduce out of plane fragments to main fragments superiorly and inferiorly • Transverse or vertical fractures require 3.5mm, 4.0mm, or 4.5mm cortical screws – Retrograde insertion of screws may be technically easier
Cannulated Lag-Screw With Tension Band (TBS) • Partially threaded cannulated screws (4.0mm) • Wire through screws and across anterior patella in figure of eight tension band • Make sure tip of screw remains buried in bone so it will not compromise wire
Cannulated Lag-Screw With Tension Band • More stable construct – Screws and tension band wire combination eliminates both possible separation seen at the fracture site with K wire/TBW and screw failure due to excessive three point bending
Suture vs. Wire Tension Band Patel et al, Injury 2000 McGreal et al, J Med Eng Tech, 1999 • Cadaveric models • Quality and stability of fixation comparable to wire • Conclude suture an acceptable alternative Gosal et al Injury 2001 • Wire v. #5 Ethibond • 37 patients • Reoperation 38% wire group vs. 6% • Infection 3 pts wire group vs. 0
Partial Patellectomy • Indicated for fractures involving extensive comminution not amenable to fixation • Larger fragments repaired with screws to preserve maximum cartilage • Smaller fragments excised – Usually involving the distal pole
Partial Patellectomy • Tendon is attached to fragment with nonabsorbable suture passed through drill holes in the fragment – Drill holes should be near the articular surface to prevent tilting of the patella • Load sharing wire passed through drill holes in the tibial tubercle and patella may be used to protect the repair and facilitate early range of motion
Total Patellectomy • Indicated for displaced, comminuted fractures not amenable to reconstruction • Bone fragments sharply dissected • Defect may be repaired through a variety of techniques • Usually results in extensor lag (30°) and loss of strength (30%) – H Kaufer, JBJS
Postoperative Management • Immobilization with knee brace, WBAT in extension • Early range of motion – Based on intraoperative assessment of repair & bone quality – Active flexion with passive extension • Quadriceps strengthening – Begin when there is radiographic evidence of healing, usually around 6 weeks • Modify depending upon fracture, osteoporosis, comorbidities, tenuous fixation and/or wounds at risk
Complications • Knee Stiffness – Most common complication • Infection – Rare, depends on soft tissue compromise • Loss of Fixation – Hardware failure in up to 20% of cases • Osteoarthritis – May result from articular damage or incongruity • Nonunion < 1% with surgical repair • Painful hardware – Removal required in approximately 15%
Extensor Tendon Ruptures • Patients are typically males in their 30’s or 40’s – Patellar < 40 yo – Quadriceps > 40 yo • Mechanism – Fall – Sports “The weekend warrior” – MVA – Tendonopathies, Steroids, Renal Dialysis
Quadriceps Tendon Rupture • Typically occurs in patients > 40 years old • Usually 0-2 cm above the superior pole • Level often associated with age – Rupture occurs at the bone-tendon junction in majority of patients > 40 years old – Rupture occurs at midsubstance in majority of patients < 40 years old
Quadriceps Tendon Ruptures • Risk Factors – Chronic tendonitis – Anabolic steroid use – Local steroid injection – Inflammatory arthropathy – Chronic renal failure – Systemic disease
History • Sensation of a sudden pop while stressing the extensor mechanism (eccentric load) • Pain at the site of injury • Inability to extend the knee • Difficulty weight-bearing
Physical Exam • Effusion • Tenderness at the upper pole • Palpable defect above superior pole • Loss of extension • With partial tears, extension will be intact
Quadriceps Tendon Rupture Radiographic Evaluation • X-ray- AP, Lateral, and Tangential (Sunrise, Merchant) – Distal displacement of the patella (patella baja) • MRI – Useful when diagnosis is unclear Treatment • Nonoperative – Partial tears and strains • Operative – For complete ruptures
Operative Treatment • Reapproximation of tendon to bone using nonabsorbable sutures with tears at the muscle-tendon junction – Locking stitch (Bunnel, Krakow) with No. 5 ethibond passed through vertical bone tunnels – Repair tendon close to articular surface to avoid abnormal patellar tilting
Operative Treatment • Midsubstance tears may undergo end-to-end repair after edges are freshened and slightly overlapped – May benefit from reinforcement from distally based partial thickness quadriceps tendon turned down across the repair site (Scuderi Technique)
Treatment • Chronic tears may require a V-Y advancement of a retracted quadriceps tendon (Codivilla V- Y-plasty Technique)
Postoperative Management • Knee immobilizer, Hinged Knee Brace, or cylinder cast for 5-6 weeks • Immediate weight-bearing as tolerated • At 2-3 weeks, hinged knee brace starting with 45 degrees active range of motion with 10-15 degrees of progression each week
Complications • Rerupture • Persistent quadriceps atrophy/weakness • Loss of motion • Infection
Patellar Tendon Rupture • Less common than quadriceps tendon rupture • Associated with degenerative changes of the tendon • Rupture often occurs at inferior pole insertion site
Patellar Tendon Rupture • Risk Factors – Rheumatoid arthritis – Systemic Lupus Erythematosus – Diabetes – Chronic Renal Failure – Systemic Corticosteroid Therapy – Local Steroid Injection – Chronic tendonitis
Anatomy • Patellar tendon – Averages 4 mm thick but widens to 5-6 mm at the tibial tubercle insertion – Merges with the medial and lateral retinaculum – 90% type I collagen
Blood Supply • Fat pad vessels supply posterior aspect of tendon via inferior medial and lateral geniculate arteries • Retinacular vessels supply anterior portion of tendon via the inferior medial geniculate and recurrent tibial arteries • Proximal and distal insertion areas are relatively avascular and subsequently are a common site of rupture