Download
1 / 21
300 likes | 1.23k Views
Extensor Tendons. Dr William Eley CT1 Plastic Surgery Morriston Hospital, Swansea. Objectives. Anatomy Injuries History of Repair Examination Management of Injuries. Anatomy. 12 Tendons Dorsally manoeuvres the wrist, thumb and fingers

E N D
Extensor Tendons Dr William Eley CT1 Plastic Surgery Morriston Hospital, Swansea
Objectives • Anatomy • Injuries • History of Repair • Examination • Management of Injuries
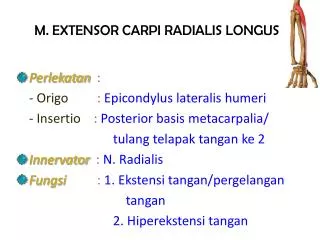
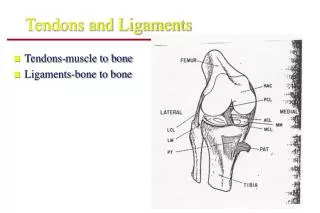
Anatomy • 12 Tendons • Dorsally manoeuvres the wrist, thumb and fingers • Participate in radial and ulnar deviation of the wrist • Involved in pronation and supination of thumb and wrist. • Primary origin – lateral humerus and proximal forearm.
Anatomy at the Wrist • 6 Compartments of extensor retinaculum. • The ERCL inserts on the dorsal base of the index metacarpal. • The ECRB inserts on the dorsal base of the long finger metacarpal. • All the extensor tendons to the hand are extrinsic, that is, no tendons that extend the digits originate in the hand.
Cont. • As the digital extensors travel over the hand, dorsum extensor juncturaetendineae are formed to cause interconnections between tendon • Juncturaetendineae can cause a misdiagnosis of an extensor tendon laceration because they can aid continual extension of a digit whose tendon was cut proximal to the juncturae. • Extensor tendons do not have flexor sheaths except for at the wrist, as tendons pass below the extensor retinaculum. • The EDC tendon to the small finger is estimated to be absent in 54% of the population.
Extensor apparatus of the finger • Complex interplay between extensor apparatus and intrinsic muscle, ligaments, volar plates and tendons • The sagittal band acts both as a static tether to prevent radial or ulnar displacement of the extensor tendon and as a dynamic tether that allows proximal and distal gliding of the extensors tendons during flexion and extension.
Injuries • Extensor tendon laceration can result from various injuries. • The most common mechanisms are • Sharp object direct laceration • Crush injury • Avulsions • Burns • Bites • Deep abrasions.
History of repair • The history of tendon reconstruction can be traced back to the times of Hippocrates and Galen. Interestingly, Galen (131-201 AD), in his ArsParva, stated that tendons were composed of both ligaments and nerves. • He warned, therefore, that placing sutures in tendons would lead to pain, twitching, and eventual convulsions. • This erroneous concept was not refuted until 1682, when Meekren observed that tendons are insensitive and described the successful repair of incompletely severed tendons. • Modern tendon repair surgery was promoted by Kirchmayr, who, in 1917, published a method of "locking" suture in tendon repair, variants of which are still in use today. • Anatomical and functional understanding of the extensor system was advanced significantly by Albinus, who first illustrated the basic structure in extensor tendon anatomy in 1734. • Further progress of extensor tendon dynamics and balance forces concepts were made by Fowler in 1942. Landsmeer also contributed to the understanding of the extensor system's dynamic interplay with the oblique retinacular ligament in 1949
Management of Injuries • Dependent on cause • Tendons thinner and of smaller calibre than flexors – cannot tolerate 2 component repair. • Figure of 8 techniques distally.
Injuries at specific levels • Distal interphalangeal joint (zone I) • Open Injuries - These injuries are invariably intra-articular. Lavage and debridement of the joint, tendon repair, skin closure, and K-wire fixation are the principles of management. A degree of hyperextension is desirable, but skin blanching should be avoided. • Remove the wire after 4 weeks and replace it with a mallet finger splint for 2 weeks. Introduce active flexion during the eighth week. • Closed Injuries - In the routine closed injury without bony involvement, use a mallet finger splint, aiming for slight hyperextension. • Zone II – repair and immobilise • Zone III - boutonnière deformity can become apparent. Repair and splint. If repaired – PIP joint in full extension. • Zone IV – Direct repair +/- k wire. • Zone V – MCPJ – Fight bites • Zone VI – Metacarpals – Matress sutures • Zone VII – Wrist – Core sutures – tendons larger.
Post op and follow up • Splint • Arrange ROS • Early mobilisation – as per protocol of centre. • For non complicated injuries (eg. single finger laceration, no associated injuries, non crush lacerations) in zone V and distally, an early active ROM protocol (of any variety) is beneficial to early patient outcome. • For multi finger, complicated injuries (eg. crush injuries with associated damaged structures) in regions proximal to zone V and in patients with compliance or extenuating social issues, immobilization for 3-4 weeks, followed by a progressive ROM exercise protocol, is preferred.
References • Henry et al. http://emedicine.medscape.com/article/1286225-overview